In line with the International Health Regulations (IHR) monitoring and evaluation framework and our organisational strategy plan, the Nigeria Centre for Disease Control (NCDC) is developing capacity in emergency preparedness and response through regular Simulation Exercises (SimEx). This is also based on the Emergency Preparedness, Resilience and Response (EPRR) strategy developed with support from Public Health England’s (PHE) IHR strengthening programme.
On the 27th and 28th of March 2019, NCDC carried out a functional stimulation exercise (“Exercise keep pushing IIâ€) on infectious disease outbreak involving State Public Health Emergency Operation Centres (PHEOCs). This is the second simulation exercise involving State PHEOCs, and has been supported by PHE.
2. Promote the understanding of NCDC’s role and responsibilities with its key stakeholders in the coordination of a public health incident
3. Assess the effectiveness of NCDC’s risk communications processes and arrangements to warn
4. Assess the effectiveness of the recently developed incident management system, SITAware within NCDC Headquarters during a public health incident
The participants included staff of NCDC, PHE, US-CDC, George Town University; NFELTP residents and NCDC trainees (interns and corps members).
In simulating a cholera outbreak, participants were involved in activation of a national EOC and constitution of a Multi-sectoral Incident Management System; development of an Incident Action Plan and Situation Report; rumour verification; notification of key stakeholders; development of a public health advisory; development of a ministerial briefing; RRT deployment; development of assessment tool for laboratory; and case management capacity of cholera treatment centers in Kebbi and Edo states.
The experience highlighted strengths including better coordination and use of EOCs, as well as limitations still experienced in incident management activation such as rapid communication. Importantly, lessons learned have been reviewed to inform further capacity development processes at the national and state level.
Through simulation exercises and other activities, NCDC continues to strengthen preparedness for outbreaks at the national and state level. It is expected that in addition to support from NCDC, states in Nigeria also strengthen their capacity to ensure sub-national health security.
SUMMARY OF REPORTS
In the reporting week ending March 17, 2019:
o There were 160 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as polio. The last reported case of polio in Nigeria was in August 2016. Active case search for AFP is being intensified with the goal to eliminate polio in Nigeria
o There were 11 suspected cases of cholera reported from four LGAs in Bayelsa State. One was laboratory confirmed and one death recorded.
o There were 79 suspected cases of Lassa fever reported from 23 LGAs in 12 States (Edo – 18, Ebonyi – 7, Ondo – 26, Bauchi -12, Enugu – 2, Gombe – 3, Imo – 1, Taraba – 6, Kebbi – 1, Katsina – 1, Kogi - 1 & Plateau – 1). Twenty-three were laboratory confirmed and four deaths were recorded.
o There were 129 suspected cases of Cerebrospinal Meningitis (CSM) reported from 33 LGAs in 15 States (Adamawa – 1, Bauchi – 1, Cross River – 1, Delta – 1, FCT – 1, Jigawa – 1, Kano – 1, Katsina – 86, Kebbi - 3, Kogi – 1, Niger – 5, Plateau – 1, Sokoto – 13, Yobe – 2 & Zamfara - 11). Of these, seven was laboratory confirmed and one death was recorded.
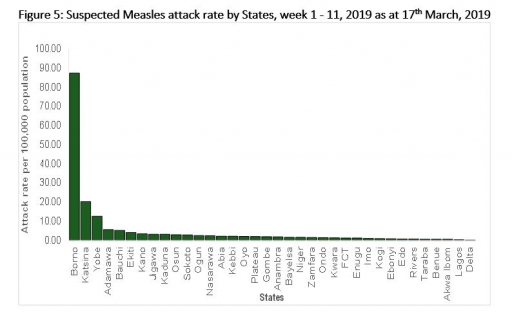
o There were 2210 suspected cases of measles reported from 36 States. Four were laboratory confirmed and four deaths were recorded.
In the reporting week, all States sent in their reports. Timeliness of reporting remained 93.0% in both weeks ten & eleven while completeness remains 99.0% at the same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1 As at March 17 2019, no new case of WPV was recorded
1.2 In the reporting week, 160 suspected cases of AFP were reported from 139 LGAs in 33 States and FCT
1.3 Between week 1 and 11 (2019), 1353 suspected cases of AFP were reported from 569 LGAs in 36 states and FCT
2. CEREBROSPINAL MENINGITIS (CSM)
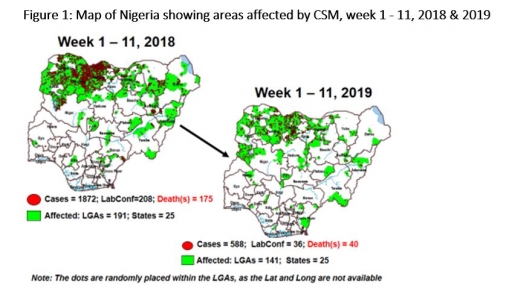
2.1 In the reporting week, 129 suspected Cerebrospinal Meningitis (CSM) cases, seven laboratory confirmed cases and one death (CFR, 0.78%) were reported from 33 LGAs in 12 States (Adamawa – 1, Bauchi – 1, Cross River – 1, Delta – 1, FCT – 1, Jigawa – 1, Kano – 1, Katsina – 86, Kebbi - 3, Kogi – 1, Niger – 5, Plateau – 1, Sokoto – 13, Yobe – 2 & Zamfara - 11) compared with 166 suspected cases with seven laboratory confirmed and 13 deaths (CFR, 7.8%) reported across 59 LGAs (16 States) at the same period in 2018 (Figure 1)
2.2 Between weeks 1 and 11 (2019), 588 suspected meningitis cases with 36 laboratory confirmed and 40 deaths (CFR, 6.8%) from 141 LGAs (25 States) were reported compared with 1872 suspected cases with 208 Laboratory confirmed and 175 deaths (CFR, 9.4%) from 191 LGAs in 25 states during the same period in 2018
2.3 Timeliness/completeness of CSM case-reporting from states to the national level (2019 versus 2018): on average, 92.4% of the 26 endemic States sent CSM reports in a timely manner while 100.0% were complete in week 1 - 11, 2019 as against 88.1% timeliness and 95.8% completeness recorded within the same period in 2018
2.4 NCDC deployed Rapid Response Team (RRT) to Katsina and Niger States
2.5 NCDC and WHO conducted training on CSF collection and enhanced surveillance for clinicians and surveillance officers in Katsina State
2.6 The CSM National Emergency Operations Centre (EOC) is on response mode and meets weekly to review the situation
2.7 CSM preparedness and response assessment checklist form sent to all States
3. CHOLERA
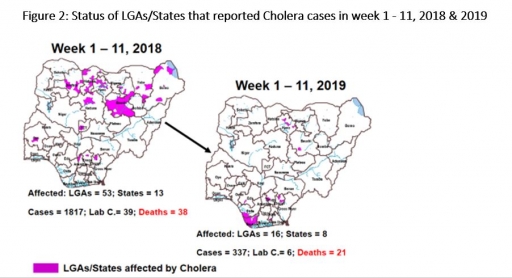
3.1 11 suspected cases of cholera with one laboratory confirmed and one death (CFR, 9.1%) were reported from four LGAs in Bayelsa State compared with 175 suspected cases with 15 laboratory confirmed and five deaths (CFR, 2.9%) reported from six LGAs in four States during the same period in 2018 (Figure 2).
3.2 Between weeks 1 and 11 (2019), 337 suspected cholera cases with six laboratory confirmed and 21 deaths (CFR, 6.23%) from 16 LGAs (eight states) were reported compared with 1817 suspected cases and 38 deaths (CFR, 2.1%) from 53 LGAs in 13 States during the same period in 2018.
3.3 NCDC deployed Rapid Respose Team (RRT) to Bayelsa State to assess the current situation
3.4 NCDC has disseminated cholera alert mails and line list template to all states in preparedness for dry season transmission
3.5 NCDC is supporting ongoing Oral Cholera vaccination campaign (28th March – 3rd April) through supervision in Michika LGA, Adamawa State.
3.6 National Preparedness and Response to Acute Watery Diarrhoea/Cholera Guidelines. Available from
http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
4 LASSA FEVER
4.1 In the reporting Week 11 (11th – 17th March, 2019), twenty-three new confirmed I cases were reported from nine States - Edo (8), Ondo (4), Ebonyi (3), Bauchi (3), Taraba (1), Imo (1), Enugu (1), Benue (1) and Kebbi (1) States with four new deaths in Edo (2), Bauchi (1) and Benue (1) States.
4.2 From 1st January – 17th March 2019, a total of 1801 suspectedi cases have been reported from 21 States including FCT. Of these, 495 were confirmed positive, 15 probable and 1277 negatives (not a case).
4.3 Since the onset of the 2019 outbreak, there have been 114* deaths among confirmed cases. Case Fatality Rate in confirmed cases is 23.0%
4.4 Twenty-one states have recorded at least one confirmed case across 73 LGAs (Edo, Ondo, Bauchi, Nasarawa, Ebonyi, Plateau, Taraba, FCT, Adamawa, Gombe, Kaduna, Kwara, Benue, Rivers, Kogi, Enugu, Imo, Delta, Oyo, Kebbi & Cross River) and remain active.iv
4.5 NCDC deployed RRT to Taraba State to access the current situation & support the State team
4.6 Assessment of the two treatment centres in Plateau state by NCDC case management team
4.7 NCDC provided an ambulance to the Infection Control Centre of Federal Medical Centre Owo
4.8 NCDC prepositioned PPEs, Ribavirin (injection and tablets), beds, Tents, body-bags, thermometers, hypochlorite hand sanitizers, IEC materials, guidelines and SOPS distributed across 36 states, FCT and treatment centres
4.9 A National Lassa fever multi-partner, multi-sectoral Emergency Operational Centre (EOC) continues to coordinate the response activities at all levels. State EOCs have also been activated in Edo, Ondo, Plateau, Kebbi and Ebonyi

5 MEASLES
5.1 In the reporting week, 2210 suspected cases of measles with four laboratory confirmed cases and four deaths (CFR, 0.18%) were reported from 36 states compared with 605 suspected cases and two deaths (CFR,0.33%) reported from 34 states during the same period in 2018
5.2 Since the beginning of the year, 11603 suspected measles cases with 535 laboratory confirmed and 27 deaths (CFR, 0.23%) were reported from 36 states and FCT compared with 4764 suspected cases and 34 deaths (CFR, 0.71 %) from 36 States and FCT, during the same period in 2018
5.3 Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards and LGAs during Supplementary Immunization Activities (SIAs), as well as case management
5.4 NCDC deployed Rapid Respose Team (RRT) to Yobe State to access the current situation
5.5 A National Measles multi-partner, multi-sectoral Emergency Operational Centre (EOC) activated on the 10th March, 2019 to coordinate response activities
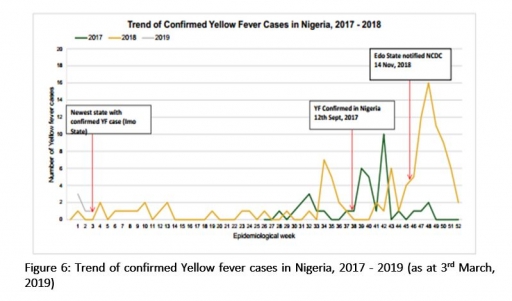
6 Yellow fever
6.1 In the reporting week 9 (24th February – 3rd March, 2019), eight suspected yellow fever cases were recorded in Nigeria
6.2 No new confirmed case from Institute Pasteur (IP) Dakar and the last IP Dakar confirmed cases was on the 20th of February 2019
6.3 From 1st January – 3rd March 2019, 364 suspected cases have been recorded from 177 LGAs across the country with blood samples collected from all cases. Of these, five were confirmed positive with no death recorded so far.
6.4 From the onset of this outbreak on September 12, 2017 to date, 4,100 suspected cases were reported from 604 (78.0%) LGAs in all the 36 States and FCT
6.5 A total of 139 cases have been confirmed by IP Dakar from 17 states (Kwara (8), Kogi (10), Kano (1), Zamfara (19), Kebbi (7), Nasarawa (3), Niger (1), Katsina (2), Edo (69), Ekiti (2), Rivers (1), Anambra (1), FCT (10), Benue (1), Delta (1), Ondo (2) and Abia (1) States) in 46 Local Government areas (LGAs).
6.6 Since the onset of the outbreak, 80 deaths were recorded among all cases with 29 deaths among IP Dakar confirmed cases. Case Fatality Rates (CFR) in all cases (suspected, probable & confirmed) and among IP Dakar confirmed cases is 2.0% and 21. 0% respectively
6.7 Yellow fever reactive vaccination campaigns were conducted in the following States: Edo (13 LGAs), Kebbi (7 LGAs), Niger (5 LGAs), Sokoto (1 LGA) &
6.8 Yellow fever vaccination campaigns have been successfully completed in 12 States (Nasarawa, Cross River, Akwa-Ibom, Kogi, Kwara, Zamfara, Sokoto, Kebbi, Niger, FCT, Plateau & Borno) and 57 political wards in 25 LGAs in Borno State. Another campaign to commence in Vandekeiya LGA in Benue State
6.9 A multi-agency national Emergency Operations Centre is coordinating the national response
6.9.1 Yellow fever After Action Review (AAR) being planned and is slated for April 2019
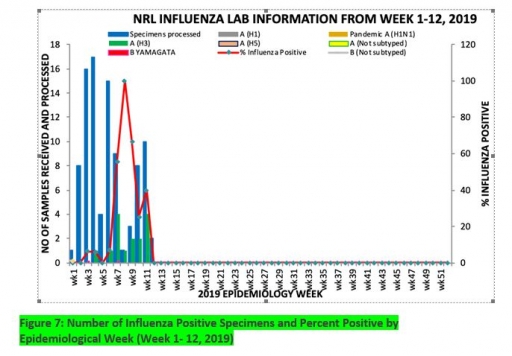
7. Update on national Influenza sentinel surveillance, Nigeria week 1 – 12, 2019
7.1 From week 1- 12 2019, a total of 94 samples were recruited, of which 89 were Influenza like-illness (ILI) and five was Severe Acute Respiratory Infection (SARI) .
7.2 A total of 94 samples were received and all samples were processed. Of the processed samples, 89(94.7%) were ILI cases and 5 (5.3%) was Severe Acute Respiratory Infection (SARI).
7.3 Of the 89 processed ILI samples, 12(13.5%) were positive for Influenza A; 2(2.3%) was positive for Influenza B and 75 (84.3%) were negative.
7.4 For the processed five SARI samples, 3(60.0%) were positive for Influenza A, 0(0.0%) for Influenza B and 2(40.0%) were negative.
7.5 Of the 89 processed samples, 17 (19.1%) were positive for Influenza, with 15 (88.2%) of these positive for Influenza A and 2 (11.8%) positive for Influenza B.
7.6 The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for 15 (100.0%), 0 (0.0%) and 0 (0.0%) of the total influenza A positive samples respectively.
7.7 The subtypes B VICTORIA, B Not subtyped and B Yamagata account for 0(0.0%), 2(100.0%) and 0(0.0%) of the total influenza B positive samples respectively
7.8 The percentage of influenza positive was highest (100.0%) in week 8, 2019
7.9 In the reporting week 1- 12, all samples were duely processed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
