As at the 19th of October 2017, 74 suspected cases of Monkeypox have been reported from 11 states, including the Federal Capital Territory (FCT). In Epi-week 42, results of samples sent for testing were received in the country. Of the 17 samples sent from Bayelsa state, three were positive for monkey pox virus, 12 were negative and 2 results are still pending. Results of four samples sent from Lagos state all turned out negative for monkey pox virus. Samples sent from other states are being awaited
The availability of the laboratory results has, by all definitions, provided evidence for confirmation of the outbreak in Bayelsa state. In addition, this will support case identification which are epidemiologically linked and initiate proper clinical management. This week’s editorial will focus on managing confirmed cases of monkey pox as well as prevention of the disease.
Currently, there is no known treatment for monkey pox disease. However, the following steps should be taken in management of a confirmed case:
1. Isolation of patient-An isolation centre /unit should be set up to manage cases of monkey pox disease. This will help minimize transmission of infection through body contact
2. Use of Personal Protective Equipment (PPE)-It is advisable to use PPEs during the course of managing a case of monkey pox disease
3. Infection Prevention and Control measures should be employed at all times during the management of cases
4. Supportive therapy-Anti-pyretics for fever, analgesics for headache and body pains, care of crusts following appearance of skin manifestation of the disease
As seen with most viral infections, monkey pox disease is self-limiting and will run its course, which is for about two weeks.
1. Preventing spread of the virus through restrictions on animal trade: Potentially infected animals should be isolated from other animals and placed into immediate quarantine. Animals that may have come in contact with an infected animal should be quarantined, handled with standard precautions and observed for monkeypox symptoms for 30 days
2. Reducing the risk of infection in people: During human monkeypox outbreaks, close contact with other patients is the most significant risk factor for transmission of infection. In the absence of specific treatment or vaccine, the only way to reduce infection in people is by raising awareness of the risk factors and educating people about the measures they can take to reduce exposure to the virus. Surveillance measures and rapid identification of new cases is critical for outbreak containment
3. Controlling infection in health-care settings: Health-care workers caring for patients with suspected or confirmed monkey pox virus infection, or handling specimens from them, should implement standard infection control precautions. Samples taken from people and animals with suspected monkey pox virus infection should be handled by trained staff working in suitably equipped laboratories
The Nigeria Centre for Disease Control (NCDC) in collaboration with its partners has continued to coordinate outbreak response activities in the states. Response activities have been enhanced in Bayelsa states following laboratory confirmation. States are enjoined to continue to sensitise the public on the disease and to carry out trainings/refresher trainings on infection prevention and control measures for healthcare workers. More information on Monkey pox can be found on http://ncdc.gov.ng/news/106/05-october-2017-%7C-monkeypox-advisory
1. cdc.gov/poxvirus/monkeypox
2. www.who.int
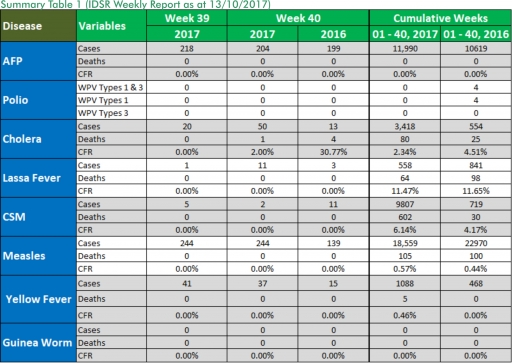
In the reporting week ending on the 8th of October, 2017:
o There were 204 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has assiduously reinvigorated its efforts at eradicating Polio.
o 50 suspected cases of Cholera were reported from four LGAs (four States; Bauchi – 3, Borno – 35, Kaduna – 4 and Zamfara – 8). None was laboratory confirmed and one death was recorded.
o 11 suspected cases of Lassa fever were reported from eight LGAs in (eight State: Bauchi – 1, Benue – 2, FCT – 1, Katsina – 2, Kogi – 1, Kwara – 2, Ogun – 1 & Plateau -1). One was laboratory confirmed (Plateau) and no death was recorded.
o There were two suspected cases of Cerebrospinal Meningitis (CSM) reported from two LGAs in two States (Ebonyi – 1 and Plateau - 1). Of these, none was laboratory confirmed and no death was recorded. Ongoing surveillance for CSM has been intensified in all the 26 States in the Nigeria meningitis belt.
o There were 244 suspected cases of Measles reported from 34 States. None was laboratory confirmed and no death was recorded.
In the reporting week, Kaduna State failed to send in their report. Timeliness of reporting remains 84% in both previous and current weeks (Week 39 and 40) while completeness remains at 100%. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
1. LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
1.1. 11 suspected cases of Lassa fever with one laboratory confirmed, were reported from eight LGAs (eight States; Bauchi – 1, Benue – 2, FCT – 1, Katsina – 2, Kogi – 1, Kwara – 2, Ogun – 1 & Plateau -1) in week 40, 2017 compared with three suspected cases reported from three LGAs (three States) at the same period in 2016.
1.2. Laboratory results of the 11 suspected cases were positive for Lassa fever (Plateau – 1) and ten negatives for Lassa fever & other VHFs (Bauchi – 1, Benue – 2, FCT – 1, Katsina – 2, Kogi -1 & Ogun -1).
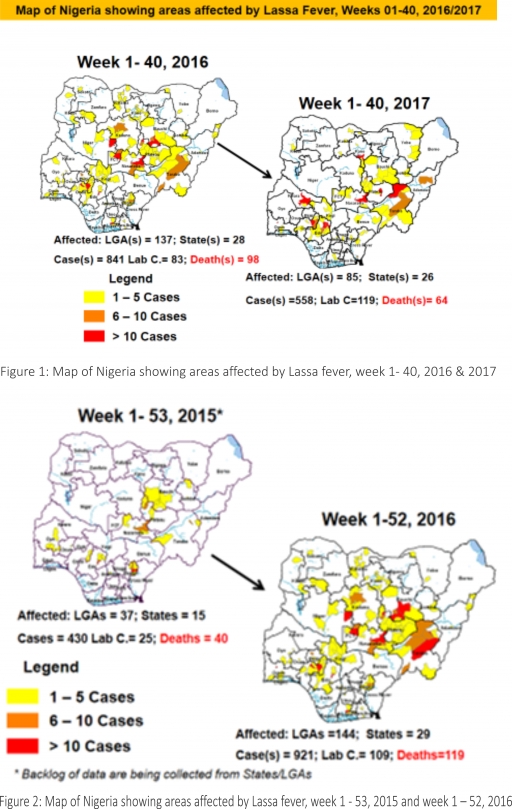
1.3. Between weeks 1 and 40 (2017), 558 suspected Lassa fever cases with 119 laboratory confirmed cases and 64 deaths (CFR, 11.47%) from 85 LGAs (26 States) were reported compared with 841 suspected cases with 83 laboratory confirmed cases and 98 deaths (CFR, 11.65%) from 137 LGAs (28 States) during the same period in 2016 (Figure 1).
1.4. Between weeks 1 and 52 2016, 921 suspected Lassa fever cases with 109 laboratory confirmed cases and 119 deaths (CFR, 12.92%) from 144 LGAs (28 States and FCT) were reported compared with 430 suspected cases with 25 laboratory confirmed cases and 40 deaths (CFR, 9.30%) from 37 LGAs (14 States and FCT) during the same period in 2015 (Figure 2).
1.5. Investigation and active case search ongoing in affected States with coordination of response activities by the NCDC with support from partners.
1.5.1. National Lassa Fever Working Group meeting and weekly National Surveillance and Outbreak Response meeting on-going at NCDC to keep abreast of the current Lassa fever situation in the country.
1.5.2. Response materials for VHFs provided to support States
1.5.3. New VHF guidelines have been developed by the NCDC (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) and are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
1.5.4. VHF case-based forms completed by affected States are being entered into the new VHF management system. This system allows for the creation of a VHF database for the country.
1.5.5. Confirmed cases are being treated at identified treatment/isolation centres across the States with Ribavirin and necessary supportive management also instituted
1.5.6. Onsite support was earlier provided to Ogun, Nasarawa, Taraba, Ondo and Borno States by the NCDC and partners
1.5.7. Offsite support provided by NCDC/partners in all affected States
1.5.8. States are enjoined to intensify surveillance and promote Infection, Prevention and Control (IPC) measures in health facilities.
2. MEASLES
2.1. In the reporting week, 244 suspected cases of Measles were reported from 34 States compared with 139 suspected cases reported from 22 States during the same period in 2016.
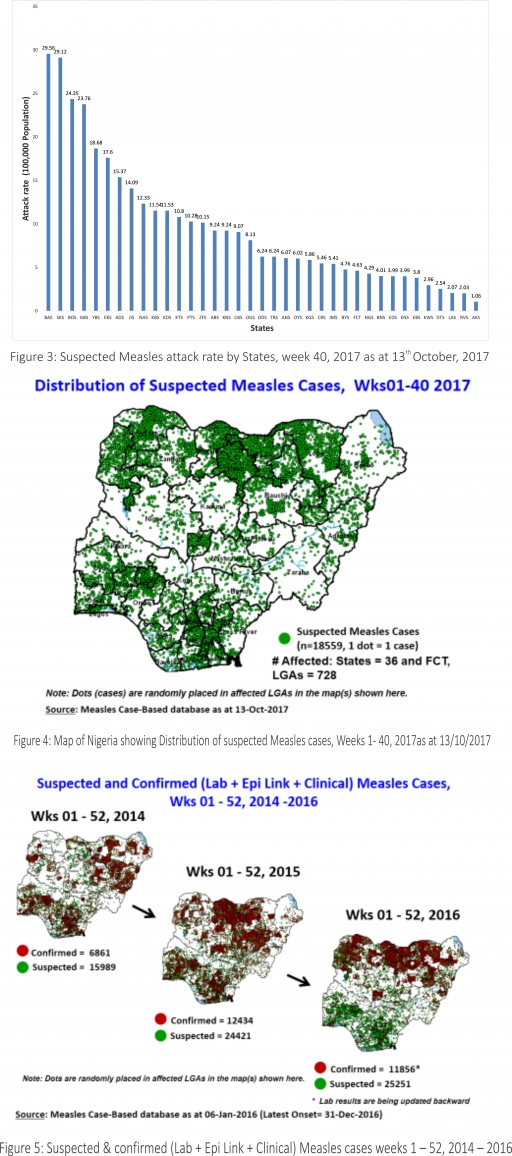
2.2. So far, 18,559 suspected Measles cases with 108 laboratory confirmed cases and 105 deaths (CFR, 0. 56%) have been reported in 2017 from 36 States and FCT (Figure 4) compared with 22,970 suspected cases and 100 deaths (CFR, 0.44%) from 36 States and FCT during the same period in 2016.
2.3. In 2016 (week 1 -52), 25,251 suspected Measles cases with 102 deaths (CFR, 0.40%) were reported from 36 States and FCT compared with 24,421 suspected cases with 127 deaths (CFR, 0.52%) during the same period in 2015 (Figure 5)
2.4. Response measures include immunisation for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management.
2.5. Scheduled Measles campaigns in the North East were conducted from 12th – 17th January 2017 in Adamawa, Borno and Yobe States (Phase I) and Phase II from 21st – 25th January 2017 in Borno State and 4th – 8th February 2017 in Yobe State
2.6. Measles Surveillance Evaluation and Establishment of the burden of Congenital Rubella Syndrome (CRS) in 12 selected States in the six geopolitical zones from the 17th -21st July 2017 conducted
2.6.1 Debrief meeting to review results and next steps from Measles evaluation conducted, held on the 15th of September 2017
2.7. Harmonisation of measles surveillance data with laboratory-confirmed cases
3. POLIOMYELITIS
3.1. As at October 6th, 2017, no new case of WPV was recorded
3.2. Three new cVDPV2, environmental derived and Polio compatible cases identified
3.2.1. In the reporting week, 204 cases of AFP were reported from 159 LGAs in 33 States and FCT
3.2.2. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
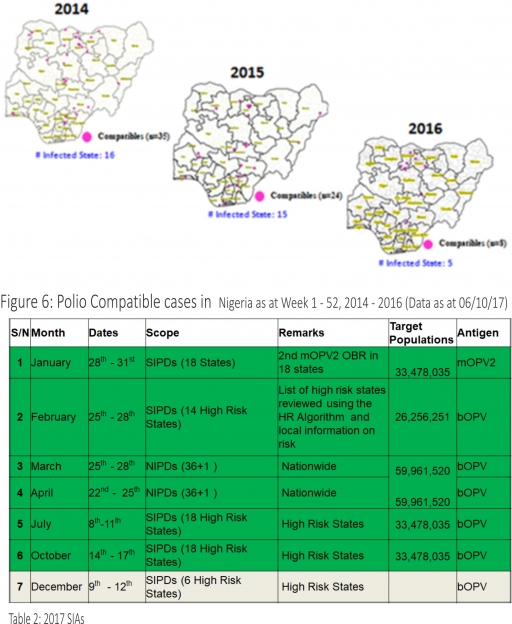
3.2.3. The 1st round of SIPDs in 2017 was conducted from 28th – 31st January 2017 in the 18 high-risk States. This was carried out using mOPV2 (2nd mOPV2 OBR). The schedule for other SIAs is as described in Table 2
3.2.4. The 2nd and 3rd round of SIPDs completed (25th-28th February and 8th – 11th July 2017) in 14 & 18 high-risk States using bOPV respectively.
3.2.5. The 1st and 2nd rounds of NIPDs completed (from 25th – 28th March 2017 and 22nd – 25th April 2017) nationwide respectively.
3.2.6. The 4th round of SIPDs completed from 14th- 17th October 2017 in 18 high-risk States using bOPV.
3.2.7. Between weeks 1 and 52 in 2016, four WPVs were isolated from Borno State compared to no WPV isolated during the same period in 2015.
3.3. No circulating Vaccine Derived Polio Virus type 2 (cVDPV2) was isolated in week 1 - 52, in both 2016 and 2015.
3.4. Between weeks 1 and 52, 2016 two (2) cVDPV2 were isolated in two LGAs (two States) while one (1) cVDPV2 was isolated from Kwali, FCT during the same period in 2015.
3.5. Six confirmed WPVs were isolated in 2014.
3.6. The SIAs were strengthened with the following events:
3.6.1. Immunisation for all vaccine-preventable diseases in some selected wards/LGAs.
3.6.2. Use of health camp facilities.
3.6.3. Field supportive supervision and monitoring.
3.6.4. Improved Enhanced Independent Monitoring (EIM) and Lots Quality Assessments (LQAs) in all Polio high-risk States.
3.6.5. High level of accountability framework
4. CHOLERA
4.1. 50 suspected cases of Cholera and one death (CFR, 2.0%) were reported from eight LGAs (eight States; Bauchi – 3, Borno – 35, Delta – 3, Kaduna - 4 and Zamfara – 8) in week 40 compared with 13 suspected cases and four deaths (CFR, 1.5%) reported from two LGAs in two States during the same period in 2016.
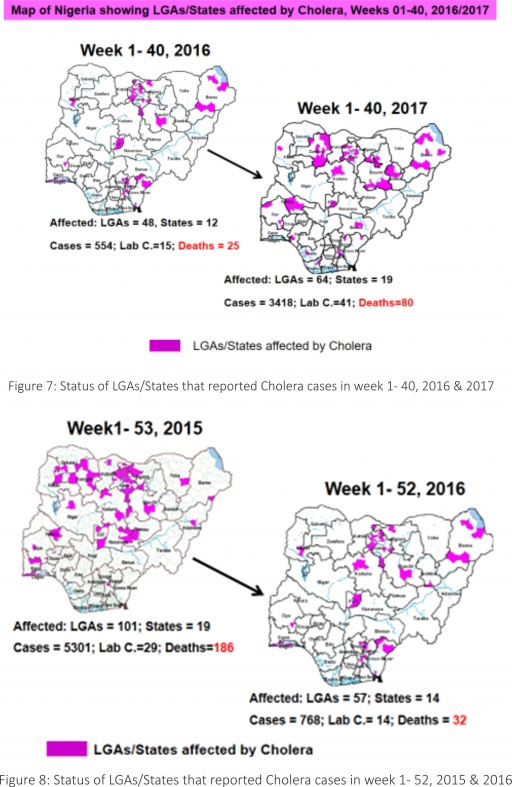
4.2. Between weeks 1 and 40 (2017), 3418 suspected Cholera cases with 41 laboratory confirmed and 80 deaths (CFR, 2.34%) from 64 LGAs (19 States) were reported compared with 554 suspected cases and 25 deaths (CFR, 4.51%) from 48 LGAs (12 States) during the same period in 2016 (Figure 7).
4.3. Between weeks 1 and 52 (2016), 768 suspected Cholera cases with 14 laboratory confirmed cases and 32 deaths (CFR, 4.17%) from 57 LGAs (14 States) were reported compared with 5,301 cases with 29 laboratory confirmed cases and 186 deaths (CFR, 3.51%) from 101 LGAs (18 States and FCT) during the same period in 2015 (Figure 8).
4.4. Cholera preparedness workshop held from 31st May – 1st June 2017 in Abuja to
develop Cholera preparedness plan as the season set in.
4.5. NCDC/partners provided onsite support in Kwara, Zamfara and Kebbi States.
4.6 NCDC/partners are providing onsite support in Borno State.
4.7. Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines have been finalized: http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
4.8. RDT procured by NCDC and WHO prepositioned in affected States
4.9 States are enjoined to intensify surveillance, implement WASH activities and ensure early reporting.
5. CEREBROSPINAL MENINGITIS (CSM
5.7. In the reporting week 40, two suspected Cerebrospinal Meningitis (CSM) cases were reported from two LGAs (two States) compared with 11 suspected cases from seven LGAs (five States) at the same period in 2016.
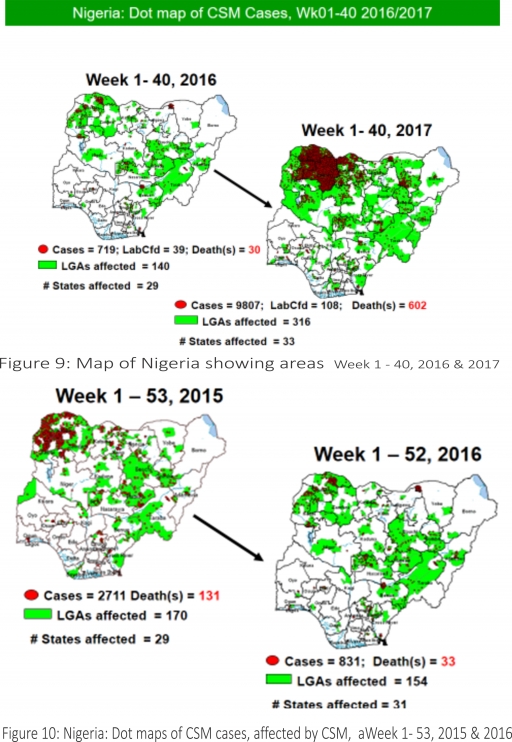
5.8. Between weeks 1 and 40 (2017), 9807 suspected CSM cases with 108 laboratory confirmed cases and 602 deaths (CFR, 6.14%) were recorded from 315 LGAs (33 States) compared with 719 suspected cases and 30 deaths (CFR, 4.17%) from 140 LGAs (29 States) during the same period in 2016 (Figure 9).
5.9. Between weeks 1 and 52, 2016, 831 suspected CSM cases with 43 laboratory confirmed cases and 33 deaths (CFR, 3.97%) were recorded from 154 LGAs (30 States and FCT) compared with 2,711 suspected cases and 131 deaths (CFR, 4.83%) from 170 LGAs (28 States and FCT) during the same period in 2015 (Figure 10)
5.10. Timeliness/completeness of CSM case-reporting from States to the National Level (2017 versus 2016): on average, 82.2% of the 26 endemic States sent CSM reports in a timely manner while 98.6% were complete in week 1 – 40, 2017 as against 86.0% timeliness and 99.6% completeness recorded within the same period in 2016
5.11. NCDC attended the 14th Annual Meeting on Surveillance, Preparedness and Response to Meningitis Outbreaks in Africa, and 4th Annual MenAfriNet Partners’ meeting held in Ouagadougou, Burkina Faso in preparation of 2017/2018 meningitis season from 12th to 15th September 2017.
5.12. Ongoing finalisation of the National CSM Guidelines
5.13. Enhanced surveillance to begin 1st of December 2017, ahead of the 2017/2018 dry season
5.14. Development of State-specific CSM Epidemic Preparedness & Response plan ongoing in 11 Northern States within the Meningitis belt
6. GUINEA WORM DISEASE
6.7. In the reporting week, no rumour report of Guinea Worm disease was received from any State.
6.8. Nigeria has celebrated eight consecutive years of zero reporting of Guinea worm disease in the country. The Country has been officially certified free of Dracunculiasis transmission by the International Commission for the Certification of Dracunculiasis Eradication (ICCDE).
(For further information, contact Nigeria Guinea Worm Eradication Program / Neglected Tropical Diseases Division, Public Health Department/Federal Ministry of Health)
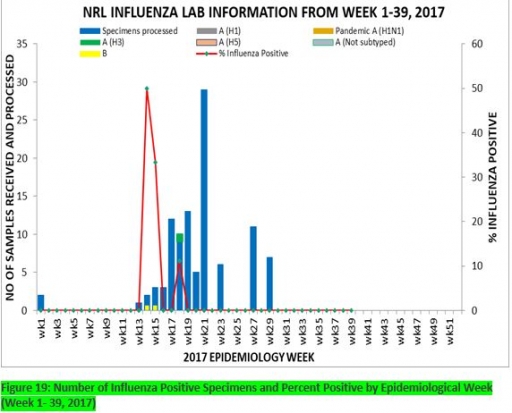
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 39, 2017
7.1. From week 1-39, a total of 103 suspected cases were reported, of which 95 were Influenza like-illness (ILI), 8 Severe Acute Respiratory Infection (SARI).
7.2 A total of 103 samples were received and all were processed. Of the processed samples, 95(92.2%) were ILI cases, 8(7.8%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 95 processed ILI samples, 1(1.05%) was positive for Influenza A; 2(2.1%) positive for Influenza B and 92(98.95%) were negative. Of the 8 processed SARI samples, none was positive for Influenza A and Influenza B.
7.5. In the reporting week 39, no samples were left unprocessed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
