In the last few months, Nigeria has experienced outbreaks of Cholera, Lassa fever, and most recently Monkeypox. The response and coordination of these outbreaks define their outcome. As with all events of importance, outbreaks are usually rife with stories, some of which are unfounded and may create panic. This week’s editorial focuses on the importance of messages and information provided during an outbreak. This is also important in informing better decision making and outbreak response efforts. Some important points to note are listed below:
1. Outbreaks are urgent public health emergency events and are usually accompanied by rapid efforts to care for cases and prevent further spread. These usually require prompt, life-saving decisions and response, with support from an informed public.
2. Outbreaks are usually alarming events that can elicit great anxiety in the public. The anxiety created usually manifests in extremes of behaviours like mask-wearing, avoidance of travel, loss of trust and confidence in government, patient stigmatization and fear of hospitals. It is therefore important that government officials responsible provide the public with information, and the media supports dissemination of approved information.
3. Outbreaks are socially and economically disruptive which arise from public reactions to information shared about the outbreak. With social disruption and economic losses, more attention is focused on the outbreak. This, in itself, can become an advantage as it could set the tone for political commitment to outbreak control including adequate resources and high level support for intervention. On the other hand, outbreak control can be impeded when political authorities, if motivated by economic rather than public health concerns, decide to withhold information about an outbreak, downplay its significance or conceal its existence. This can endanger the health of people.
4. Outbreaks are clearly news worthy events which are followed closely by national and international media, with several implications for outbreak control. On the positive side, the media can play a very pivotal role at the start of an outbreak as a tool for information sharing with the public. This has an advantage of generating more public interest and collaboration, providing a platform for informed decision making when technical reports are provided and alleviating the intending anxiety and general panic that may ensue.
The Nigeria Centre for Disease Control (NCDC) as part of its responsibilities has utilised various media channels to create awareness and enlighten the public on various disease outbreaks in the country. The agency through various mass and print media channels, social media platforms, its website and connect centre has continued to disseminate information to all concerned.
States and the general public at large are encouraged to utilise these platforms to encourage sharing of authentic information and also a means of seeking clarifications. Situation reports and other information on all disease outbreaks can be found on www.ncdc.gov.ng.
1. www.who.int/csr
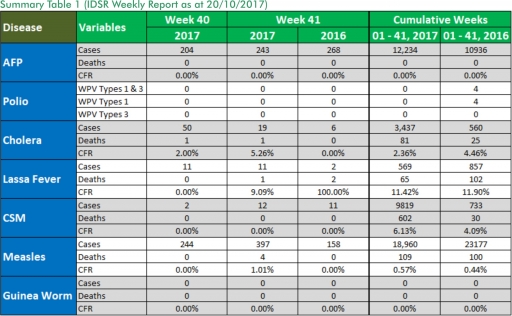
In the reporting week ending on the 15th of October, 2017:
o There were 243 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has assiduously reinvigorated its efforts at eradicating Polio.
o 19 suspected cases of Cholera were reported from two LGAs in Borno State). None was laboratory confirmed and one death was recorded.
o 11 suspected cases of Lassa fever were reported from six LGAs in (six States: Bauchi – 1, Edo – 3, Kogi – 1, Ogun – 1, Oyo – 1 & Plateau -4). One was laboratory confirmed (Plateau) and one death was recorded.
o There were 12 suspected cases of Cerebrospinal Meningitis (CSM) reported from seven LGAs in six States (Delta – 1, Enugu – 1, FCT – 3, Katsina – 4, Ondo - 1 and Plateau - 2). Of these, none was laboratory confirmed and no death was recorded. Ongoing surveillance for CSM has been intensified in all the 26 States in the Nigeria meningitis belt.
o There were 397 suspected cases of Measles reported from 32 States. None was laboratory confirmed and four deaths were recorded.
In the reporting week, Kaduna State failed to send in their report. Timeliness of reporting remains 84% in both previous and current weeks (Week 40 and 41) while completeness remains at 100%. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
1. LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
1.1. 11 suspected cases of Lassa fever with one laboratory confirmed and one death (CFR,9.09%) were reported from six LGAs (six States; Bauchi – 1, Edo – 3, Kogi – 1, Ogun – 1, Oyo – 1 & Plateau -4) in week 41, 2017 compared with two suspected cases and two deaths (CFR, 100%) reported from two LGAs (two States) at the same period in 2016.
1.2. Laboratory results of the 11 suspected cases were one positive for Lassa fever (Bauchi – 1) and ten negatives for Lassa fever & other VHFs (Edo – 3, Kogi – 1, Ogun – 1, Oyo – 1 & Plateau -4).
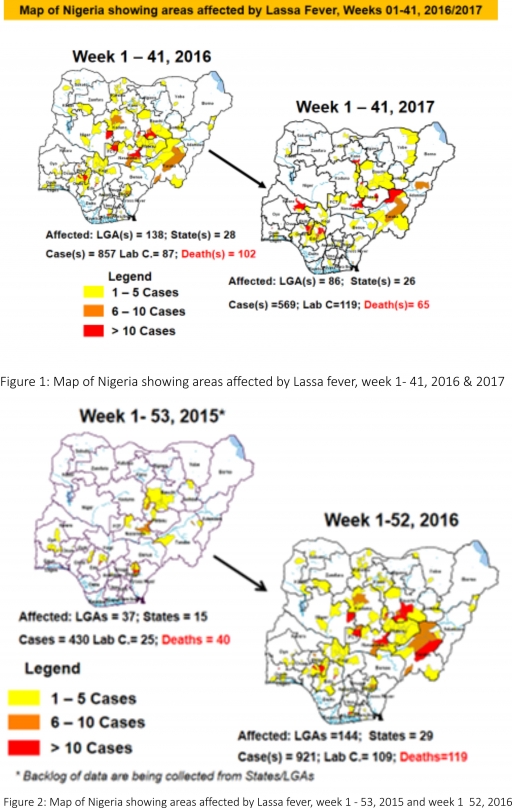
1.3. Between weeks 1 and 41 (2017), 569 suspected Lassa fever cases with 120 laboratory confirmed cases and 65 deaths (CFR, 11.42%) from 86 LGAs (26 States) were reported compared with 857 suspected cases with 87 laboratory confirmed cases and 102 deaths (CFR, 11.90%) from 138 LGAs (28 States) during the same period in 2016 (Figure 1).
1.4. Between weeks 1 and 52 2016, 921 suspected Lassa fever cases with 109 laboratory confirmed cases and 119 deaths (CFR, 12.92%) from 144 LGAs (28 States and FCT) were reported compared with 430 suspected cases with 25 laboratory confirmed cases and 40 deaths (CFR, 9.30%) from 37 LGAs (14 States and FCT) during the same period in 2015 (Figure 2).
1.5. Investigation and active case search ongoing in affected States with coordination of response activities by the NCDC with support from partners.
1.5.1. National Lassa Fever Working Group meeting and weekly National Surveillance and Outbreak Response meeting on-going at NCDC to keep abreast of the current Lassa fever situation in the country.
1.5.2. Response materials for VHFs provided to support States
1.5.3. New VHF guidelines have been developed by the NCDC (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) and are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
1.5.4. VHF case-based forms completed by affected States are being entered into the new VHF management system. This system allows for the creation of a VHF database for the country.
1.5.5. Confirmed cases are being treated at identified treatment/isolation centres across the States with Ribavirin and necessary supportive management also instituted
1.5.6. Onsite support was earlier provided to Ogun, Nasarawa, Taraba, Ondo and Borno States by the NCDC and partners
1.5.7. Offsite support provided by NCDC/partners in all affected States
1.5.8. States are enjoined to intensify surveillance and promote Infection, Prevention and Control (IPC) measures in health facilities.
2. MEASLES
2.1. In the reporting week, 397 suspected cases of Measles and four deaths (CFR, 1.01%) were reported from 32 States compared with 158 suspected cases reported from 27 States during the same period in 2016.
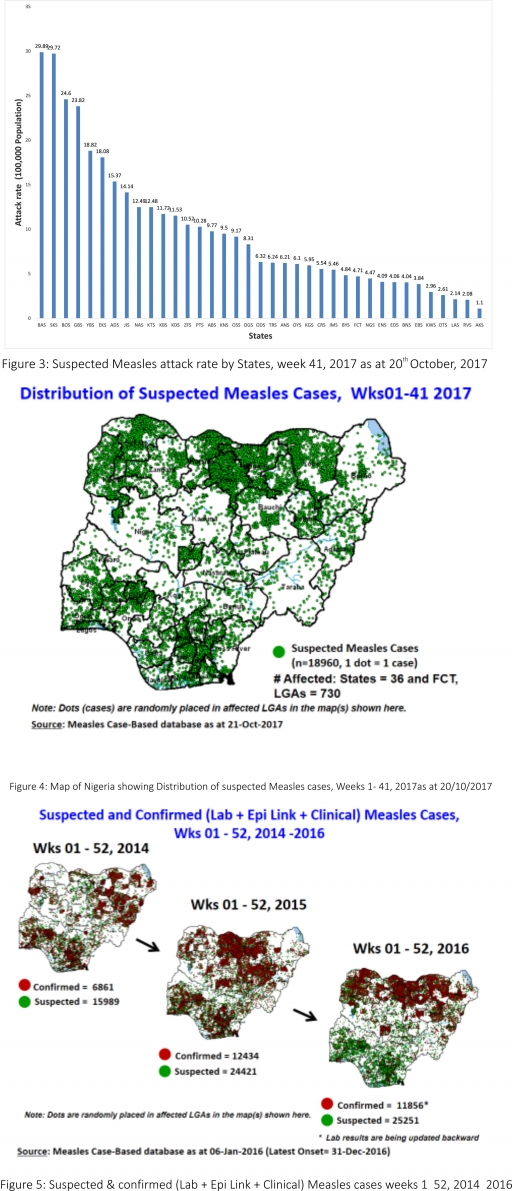
2.2. So far, 18,960 suspected Measles cases with 108 laboratory confirmed cases and 109 deaths (CFR, 0. 57%) have been reported in 2017 from 36 States and FCT (Figure 4) compared with 23,177 suspected cases and 100 deaths (CFR, 0.43%) from 36 States and FCT during the same period in 2016.
2.3. In 2016 (week 1 -52), 25,251 suspected Measles cases with 102 deaths (CFR, 0.40%) were reported from 36 States and FCT compared with 24,421 suspected cases with 127 deaths (CFR, 0.52%) during the same period in 2015 (Figure 5)
2.4. Response measures include immunisation for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management.
2.5. Scheduled Measles campaigns in the North East were conducted from 12th – 17th January 2017 in Adamawa, Borno and Yobe States (Phase I) and Phase II from 21st – 25th January 2017 in Borno State and 4th – 8th February 2017 in Yobe State
2.6. Measles Surveillance Evaluation and Establishment of the burden of Congenital Rubella Syndrome (CRS) in 12 selected States in the six geopolitical zones from the 17th -21st July 2017 conducted
2.6.1 Debrief meeting to review results and next steps from Measles evaluation conducted, held on the 15th of September 2017
2.7. Harmonisation of measles surveillance data with laboratory-confirmed cases
4. CHOLERA
4.1. 19 suspected cases of Cholera and one death (CFR, 5.26%) were reported from two LGAs in Borno State in week 41 compared with six suspected cases reported from Akinyele LGA in Oyo State during the same period in 2016.
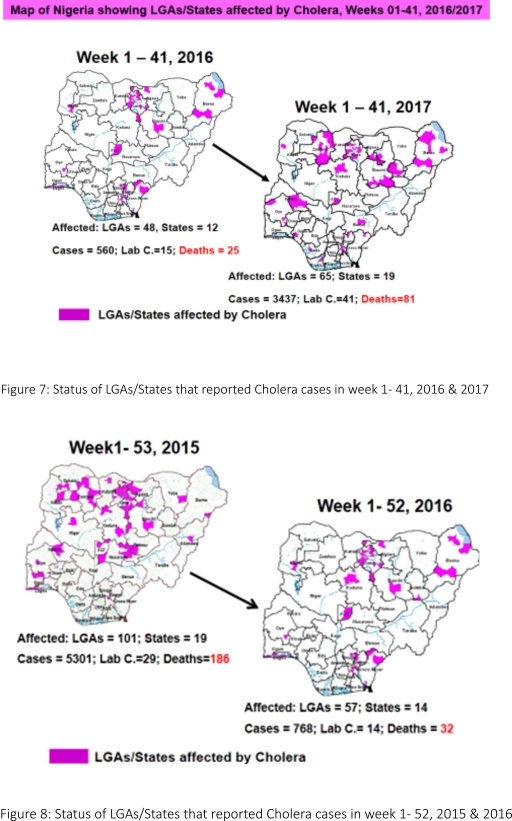
4.2. Between weeks 1 and 41 (2017), 3437 suspected Cholera cases with 41 laboratory confirmed and 81 deaths (CFR, 2.36%) from 65 LGAs (19 States) were reported compared with 560 suspected cases and 25 deaths (CFR, 4.46%) from 48 LGAs (12 States) during the same period in 2016 (Figure 7).
4.3. Between weeks 1 and 52 (2016), 768 suspected Cholera cases with 14 laboratory confirmed cases and 32 deaths (CFR, 4.17%) from 57 LGAs (14 States) were reported compared with 5,301 cases with 29 laboratory confirmed cases and 186 deaths (CFR, 3.51%) from 101 LGAs (18 States and FCT) during the same period in 2015 (Figure 8).
4.4. Cholera preparedness workshop held from 31st May – 1st June 2017 in Abuja to
develop Cholera preparedness plan as the season set in.
4.5. NCDC/partners provided onsite support in Kwara, Zamfara and Kebbi States.
4.6 NCDC/partners are providing onsite support in Borno State.
4.7. Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines have been finalized: http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
4.8. RDT procured by NCDC and WHO prepositioned in affected States
4.9 States are enjoined to intensify surveillance, implement WASH activities and ensure early reporting.
5. CEREBROSPINAL MENINGITIS (CSM)
5.7. In the reporting week 41, 12 suspected Cerebrospinal Meningitis (CSM) cases were reported from seven LGAs (six States) compared with 11 suspected cases from seven LGAs (five States) at the same period in 2016.
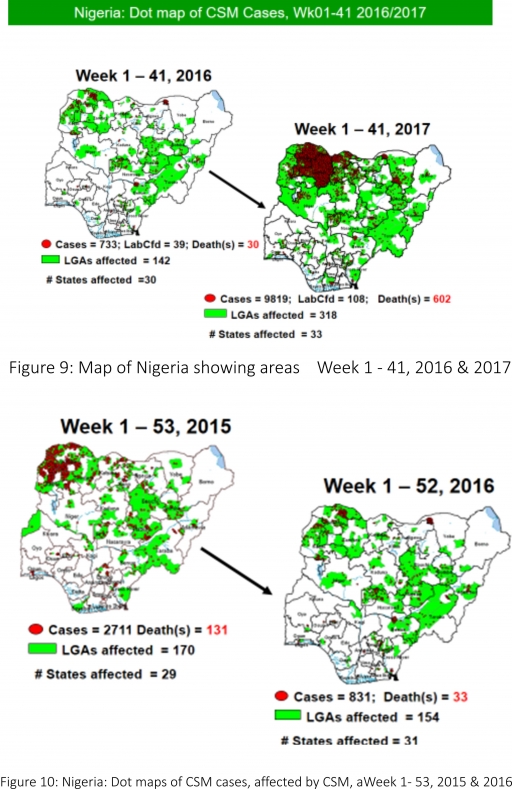
5.8. Between weeks 1 and 41 (2017), 9819 suspected CSM cases with 108 laboratory confirmed cases and 602 deaths (CFR, 6.13%) were recorded from 318 LGAs (33 States) compared with 733 suspected cases and 30 deaths (CFR, 4.09%) from 142 LGAs (30 States) during the same period in 2016 (Figure 9).
5.9. Between weeks 1 and 52, 2016, 831 suspected CSM cases with 43 laboratory confirmed cases and 33 deaths (CFR, 3.97%) were recorded from 154 LGAs (30 States and FCT) compared with 2,711 suspected cases and 131 deaths (CFR, 4.83%) from 170 LGAs (28 States and FCT) during the same period in 2015 (Figure 10)
5.10. Timeliness/completeness of CSM case-reporting from States to the National Level (2017 versus 2016): on average, 82.3% of the 26 endemic States sent CSM reports in a timely manner while 98.2% were complete in week 1 – 41, 2017 as against 85.8% timeliness and 99.4% completeness recorded within the same period in 2016
5.11. NCDC attended the 14th Annual Meeting on Surveillance, Preparedness and Response to Meningitis Outbreaks in Africa, and 4th Annual MenAfriNet Partners’ meeting held in Ouagadougou, Burkina Faso in preparation of 2017/2018 meningitis season from 12th to 15th September 2017.
5.12. Ongoing finalisation of the National CSM Guidelines
5.13. Enhanced surveillance to begin 1st of December 2017, ahead of the 2017/2018 dry season
5.14. Development of State-specific CSM Epidemic Preparedness & Response plan ongoing in 11 Northern States within the Meningitis belt
6. GUINEA WORM DISEASE
6.7. In the reporting week, no rumour report of Guinea Worm disease was received from any State.
6.8. Nigeria has celebrated eight consecutive years of zero reporting of Guinea worm disease in the country. The Country has been officially certified free of Dracunculiasis transmission by the International Commission for the Certification of Dracunculiasis Eradication (ICCDE).
(For further information, contact Nigeria Guinea Worm Eradication Program / Neglected Tropical Diseases Division, Public Health Department/Federal Ministry of Health)
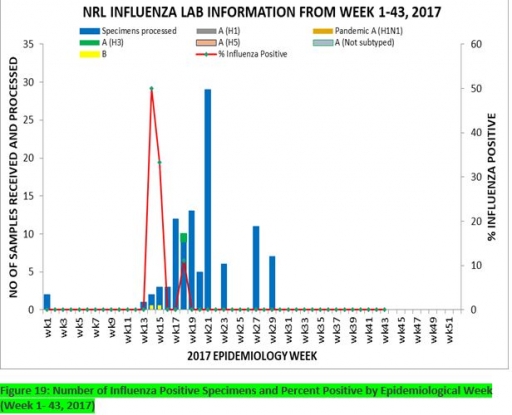
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 43, 2017
7.1. From week 1-39, a total of 103 suspected cases were reported, of which 95 were Influenza-like-illness (ILI), 8 Severe Acute Respiratory Infection (SARI).
7.2 A total of 103 samples were received and all were processed. Of the processed samples, 95(92.2%) were ILI cases, 8(7.8%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 95 processed ILI samples, 1(1.05%) was positive for Influenza A; 2(2.1%) positive for Influenza B and 92(98.95%) were negative.
7.5. Of the 8 processed SARI samples, none was positive for Influenza A and Influenza B.
7.6. The percentage influenza positive was highest (50.0%) in week 14, 2017
7.7. In the reporting week 43, no samples were left unprocessed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10

 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
