The Cholera outbreak in Kwara state continued in the Epi-week ending 9th of July with a total of 1,617 suspected cases reported, an increase of 3.6% from the last Epi-week. 13 laboratory samples were confirmed and 17 deaths recorded, giving a case fatality rate of 1.1%. The 1-5year age-group remains the most affected with a total of 460 (28.4%) cases. More males are affected, accounting for 51.6% of affected cases. 818 (50.5%) of suspected cases are reported from Ilorin West LGA of the State.
Last week’s editorial (Epi week 25) focused on the prevention of cholera through water safety. This week’s report focuses on prevention of cholera through environmental hygiene practices.
Instituting the habit of good environmental hygiene is a first step in preventing cholera outbreaks in a community or region, as the transmission cycle is not established at this point and an outbreak can be prevented.
Environmental hygiene, in this context, focuses on care of residential areas, proper treatment and disposal of waste during an outbreak.
Some preventive messages on proper environmental hygiene practices are summarized below:
1. Care of residential area
2. Waste Disposal
• Use appropriate disposal bags to gather waste before disposal.
• Use of latrines and toilets. If latrines or toilets are unavailable, bury feces 30 meters (98ft) away from any body of water.
• Increase access to improved sanitation facility e.g. connection to a public sewer, connection to a septic tank, simple pit-latrine, and ventilated improved latrine
• Facilities such as bucket latrines, public or shared latrines, and trenches should be replaced as soon as possible by improved and longer term sanitation facilities, after a cholera outbreak.
3. Treatment of Waste
• Antibacterial treatment of general sewage by chlorine, ozone, ultraviolet light or other effective treatment before it enters the waterways or underground water supplies. This helps to prevent undiagnosed cholera patients from inadvertently spreading the disease.
To achieve the maximal impact of any of the aforementioned practices, a communal approach is encouraged. This will support better fostering and impact on the general public on the importance of environmental hygiene practices, in and out of an outbreak season. These preventive messages should constitute part of the messages given to the general public at the community, LGA, State and national levels before and during an outbreak. Furthermore, healthy collaborations with the ministry of environment should be encouraged for initiating and sustaining environmental hygiene strategies implemented at all levels.
The Nigeria Centre for Disease Control (NCDC) continues to advocate for multisectoral collaboration between States and relevant Ministries, Agencies, and Departments (MDAs) and partner agencies in ensuring that a holistic approach is taken during preparation and response to outbreaks of epidemic prone diseases and public health events of concern.
Members of the public are advised to always seek care in a health facility if they have watery diarrhoea.
In the reporting week ending on the 2nd July, 2017:
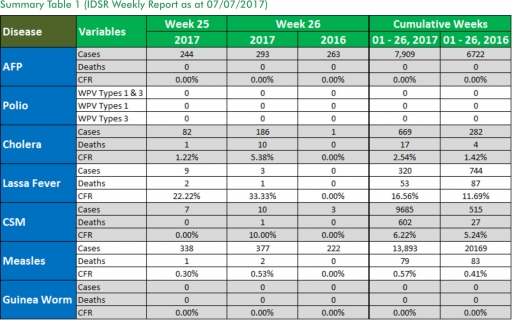
o There were 293 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has assiduously reinvigorated its efforts at eradicating Polio.
o 186 suspected cases of Cholera were reported from eight LGAs in four States with no Laboratory confirmed cases and ten deaths.
o There were ten suspected cases of Cerebrospinal Meningitis (CSM) reported from seven LGAs in five States. Of these, none was laboratory confirmed and one death was recorded. Ongoing surveillance for CSM has been intensified in the States.
o There were 377 suspected cases of Measles reported from 28 States. Six were laboratory confirmed and two deaths were recorded.
In the reporting week, Abia, Borno, Cross Rivers, Enugu, Gombe, Niger and Taraba States failed to send in any report. Timeliness of reporting remains at 82% in both previous and current weeks (Week 25 and 26) while completeness decreases from 100% to 99%. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
1. Lassa fever
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
1.1. Three suspected cases of Lassa fever with three Laboratory confirmed and one death (CFR, 33. 33%) were reported from Owo LGA (Ondo State) in week 26, 2017 compared with zero cases at the same period in 2016.
1.2. Laboratory results of the three suspected cases were three positives (Ondo - 3) for Lassa fever.
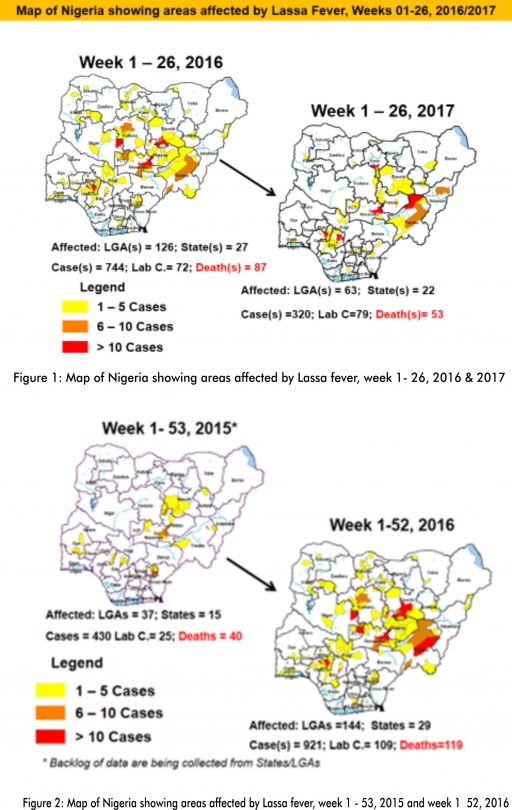
1.3. Between weeks 1 and 26 (2017), 320 suspected Lassa fever cases with 79 laboratory confirmed cases and 53 deaths (CFR, 16.56%) from 63 LGAs (22 States) were reported compared with 744 suspected cases with 72 laboratory confirmed cases and 87 deaths (CFR, 11.69%) from 126 LGAs (27 States) during the same period in 2016 (Figure 1).
1.4. Between weeks 1 and 52 2016, 921 suspected Lassa fever cases with 109 laboratory confirmed cases and 119 deaths (CFR, 12.92%) from 144 LGAs (28 States and FCT) were reported compared with 430 suspected cases with 25 laboratory confirmed cases and 40 deaths (CFR, 9.30%) from 37 LGAs (14 States and FCT) during the same period in 2015 (Figure 2).
1.5. Investigation and active case search ongoing in affected States with coordination of response activities by the NCDC with support from partners.
1.5.1. National Lassa Fever Working Group meeting and weekly National Surveillance and Outbreak Response meeting on-going at NCDC to keep abreast of the current Lassa fever situation in the country.
1.5.2. Response materials for VHFs prepositioned across the country by NCDC at the beginning of the dry season
1.5.3. New VHF guidelines have been developed by the NCDC (Interim National Viral Haemorrhagic Fevers Preparedness guidelines and Standard Operating Procedures for Lassa fever management)
1.5.4. Ongoing reclassification of reported Lassa fever cases
1.5.5. Ongoing review of the variables for case-based surveillance for VHF
1.5.6. VHF case-based forms completed by affected States are being entered into the new VHF management system. This system allows for the creation of a VHF database for the country.
1.5.7. NCDC team sent to Edo State to support Lassa fever data harmonization & Updating of VHF case-based management database
1.5.8. Confirmed cases are being treated at identified treatment/isolation centres across the States with Ribavirin and necessary supportive management also instituted
1.5.9. Onsite support was earlier provided to Ogun, Nasarawa, Taraba, Ondo and Borno States by the NCDC and partners
1.5.10. Offsite support provided by NCDC/partners in all affected States
1.5.11. NCDC and partners are providing onsite support in Ondo State, including Infection, Prevention and Control training
1.5.12. States are enjoined to intensify surveillance and promote Infection, Prevention and Control (IPC) measures in health facilities.
2. MEASLES
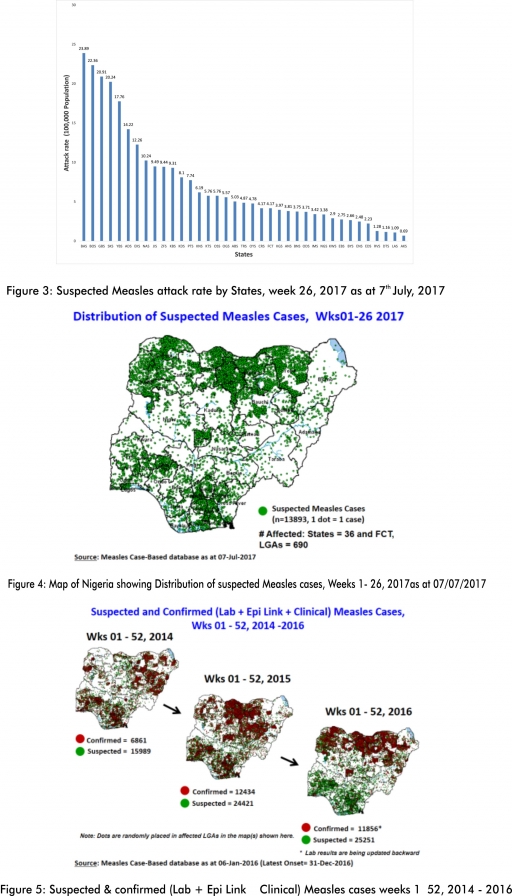
2.1. In the reporting week, 377 suspected cases of Measles with six Laboratory confirmed and two deaths (CFR, 0.30%) were reported from 28 States compared with 222 suspected measles cases from 23 States during the same period in 2016.
2.2. So far, 13,893 suspected Measles cases with 92 laboratory confirmed cases and 79 deaths (CFR, 0. 57%) have been reported in 2017 from 36 States and FCT (Figure 4) compared with 20,169 suspected cases and 83 deaths (CFR, 0.41%) from 36 States and FCT during the same period in 2016.
2.3. In 2016 (week 1 -52), 25,251 suspected Measles cases with 102 deaths (CFR, 0.40%) were reported from 36 States and FCT compared with 24,421 suspected cases with 127 deaths (CFR, 0.52%) during the same period in 2015 (Figure 5)
2.4. Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management.
2.5. Scheduled Measles campaigns in the North East were conducted from 12th – 17th January 2017 in Adamawa, Borno and Yobe States (Phase I) and Phase II from 21st – 25th January 2017 in Borno State and 4th – 8th February 2017 in Yobe State
2.6. Measles evaluation in 12 States in Nigeria to commence with National training on the 15th of July, 2017
3. POLIOMYELITIS
3.1. As at June 25th 2017, no new case of WPV was recorded
3.2. Three new cVDPV2, environmental derived and Polio compatible cases identified
3.2.1. In the reporting week, 293 cases of AFP were reported from 236 LGAs in 31 States and FCT
3.2.2. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high risk States
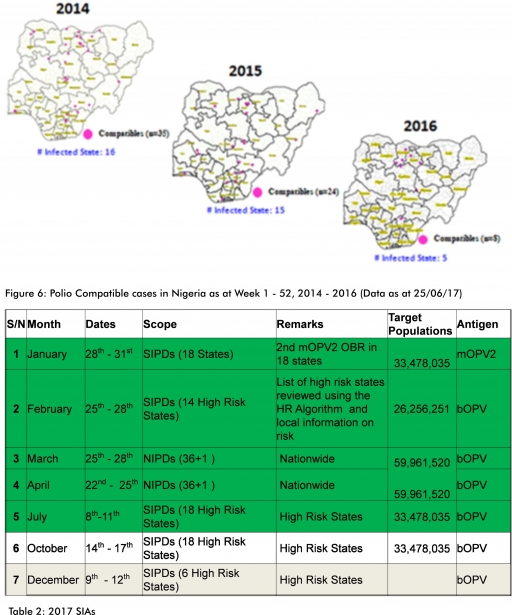
3.2.3. The 1st round of SIPDs in 2017 was conducted from 28th – 31st January 2017 in the 18 high risk States. This was carried out using mOPV2 (2nd mOPV2 OBR). The schedule for other SIAs is as described in Table 2
3.2.4. The 2nd and 3rd round of SIPDs completed (25th-28th February and 1st – 4th July, 2017) in 14 & 18 high risk States using bOPV respectively.
3.2.5. The 1st and 2nd rounds of NIPDs completed (from 25th – 28th March, 2017 and 22nd – 25th April, 2017) nationwide respectively.
3.2.6. Between weeks 1 and 52 in 2016, four WPVs were isolated from Borno State compared to no WPV isolated during the same period in 2015.
3.3. No circulating Vaccine Derived Polio Virus type 2 (cVDPV2) was isolated in week 1 - 52, in both 2016 and 2015.
3.4. Between weeks 1 and 52, 2016 two (2) cVDPV2 were isolated in two LGAs (two States) while one (1) cVDPV2 was isolated from Kwali, FCT during the same period in 2015.
3.5. Six confirmed WPVs were isolated in 2014.
3.6. The SIAs were strengthened with the following events:
3.6.1. Immunization for all vaccine-preventable diseases in some selected wards/LGAs.
3.6.2. Use of health camp facilities.
3.6.3. Field supportive supervision and monitoring.
3.6.4. Improved Enhanced Independent Monitoring (EIM) and Lots Quality Assessments (LQAs) in all Polio high risk States.
3.6.5. High level of accountability framework
4. CHOLERA
4.1. 186 suspected cases of Cholera cases and ten deaths (CFR, 1.22%) were reported from six LGAs (Kwara State) in week 26 compared with one suspected case from Lagos Island LGA (Lagos State) at the same period in 2016.
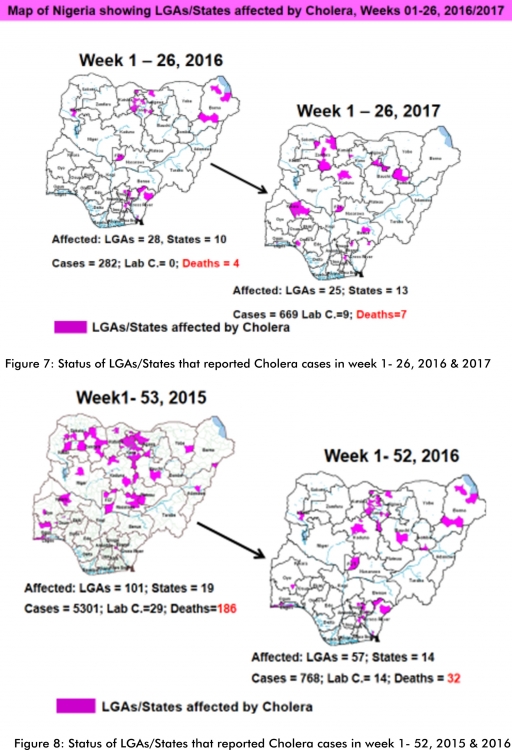
4.2. Between weeks 1 and 26 (2017), 669 suspected Cholera cases with nine laboratory confirmed and 17 deaths (CFR, 2.54%) from 25 LGAs (13 States) were reported compared with 282 suspected cases and four deaths (CFR, 1.42%) from 28 LGAs (ten States) during the same period in 2016 (Figure 7).
4.3. Between weeks 1 and 52 (2016), 768 suspected Cholera cases with 14 laboratory confirmed cases and 32 deaths (CFR, 4.17%) from 57 LGAs (14 States) were reported compared with 5,301 cases with 29 laboratory confirmed cases and 186 deaths (CFR, 3.51%) from 101 LGAs (18 States and FCT) during the same period in 2015 (Figure 8).
4.4. Cholera preparedness workshop held from 31st May – 1st June 2017 in Abuja to
develop Cholera preparedness plan as the season set in.
4.5. NCDC/partners are providing onsite support in Kwara State.
4.6. States are enjoined to intensify surveillance, implement WASH activities and ensure early reporting.
5. CEREBROSPINAL MENINGITIS (CSM)
5.1. In the reporting week 26, ten suspected Cerebrospinal Meningitis (CSM) cases and one death (CFR, 10.0%) were reported from seven LGAs (five States) compared with three suspected cases with one Lab confirmed from three LGAs (three States) at the same period in 2016.
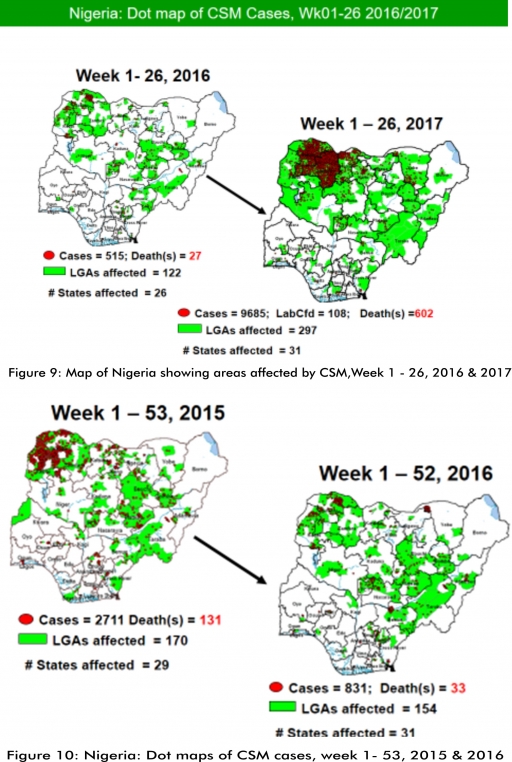
5.2. Between weeks 1 and 26 (2017), 9685 suspected CSM cases with 108 laboratory confirmed cases and 602 deaths (CFR, 6.22%) were recorded from 297 LGAs (31 States) compared with 515 suspected cases and 27 deaths (CFR, 5.36%) from 122 LGAs (26 States) during the same period in 2016 (Figure 9).
5.3. Between weeks 1 and 52, 2016, 831 suspected CSM cases with 43 laboratory confirmed cases and 33 deaths (CFR, 3.97%) were recorded from 154 LGAs (30 States and FCT) compared with 2,711 suspected cases and 131 deaths (CFR, 4.83%) from 170 LGAs (28 States and FCT) during the same period in 2015 (Figure 10)
5.4. Timeliness/completeness of CSM case-reporting from States to the National Level (2017 versus 2016): on average, 80.6% of the 26 endemic States sent CSM reports in a timely manner while 97.9% were complete in week 1 – 26, 2017 as against 83.6% timeliness and 98.1% completeness recorded within the same period in 2016
5.5. CSM preparedness checklist sent to 36 States and FCT ahead of 2017 meningitis season
5.6. Confirmed cases treated at identified treatment centres in affected States (Zamfara, Sokoto, Katsina, Kebbi, Niger, Kano, Yobe and Jigawa) and necessary supportive management also instituted
5.7. CSM National Emergency Operations Centre constituted at the Nigeria Centre for Disease Control
5.8. Onsite support provided to Zamfara, Sokoto, Katsina, Kebbi, Kano, Yobe and Niger States by NCDC and partners
5.9. Off-site support provided to other States
5.10. Intensive Surveillance in high risk States.
5.11. Reactive vaccination completed in Zamfara State for people aged one to 29 years using polysaccharide meningococcal A & C vaccine.
5.12. Reactive vaccination completed in two wards (Gada and Kaffe) in Gada LGA in Sokoto State using polysaccharide meningococcal A & C vaccine for people aged two to 29 years.
5.13. Reactive vaccination completed in nine LGAs in Sokoto State using monosaccharide meningococcal conjugate C vaccine for aged one to 20 years.
5.14. Reactive vaccination campaign completed in Yobe State for people aged two to 29 years using polyvalent ACW conjugate vaccine.
5.15. Medical teams were trained and deployed to support case management in Sokoto and Zamfara States completed (from Friday 5th - 26th May, 2017).
5.16. Deployed mobile testing laboratory to Zamfara State to aid diagnosis
5.17. A Team was deployed by NCDC/WHO to support surveillance activities, laboratory data harmonization and monitoring of the implementation plan in Yobe state
5.18. National CSM EOC has been stepped down
5.19. Evaluation of the CSM outbreak response in Zamfara and Sokoto States is ongoing by NCDC and WHO
5.20. National CSM After-Action Review meeting to be held in Sokoto State from the 24th – 25th of July 2017.
6. GUINEA WORM DISEASE
6.1. In the reporting week, no rumour report of Guinea Worm disease was received from any State.
6.2. Nigeria has celebrated eight consecutive years of zero reporting of Guinea worm disease in the country. The Country has been officially certified free of Dracunculiasis transmission by the International Commission for the Certification of Dracunculiasis Eradication (ICCDE).
(For further information, contact NIGEP NC/Director: Mrs. I, Anagbogu: +2348034085607, [email protected])
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10



 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
