Cholera is a disease condition associated with ingestion of contaminated foods and drinks and poor sanitary conditions. Control measures for Cholera outbreaks are hinged on practices of safe water use, general hygiene practices and environmental hygiene. This is based on the fact that Cholera is transmitted via faeco-oral route and preventive measures should be targeted at breaking the cycle of transmission in order to prevent and control the disease.
The focus of this report is on the prevention of cholera through safe water use and general hygiene practices. Some key preventive measures targeted at these practices have been identified and are listed in the table below:
2. Use of safe water
3. Hand Washing
4. Good Sanitary Practices
5. Safe Cooking Practices
6. Personal Hygiene
1.
• Bottled water with unbroken seals and canned/bottled carbonated beverages, registered by NAFDAC are safe to drink and use.
• Boil or treat drinking water with a chlorine product.
• If boiling, bring water to a complete boil for at least 1 minute.
• If a chlorine treatment product is not available, household bleach can be used to treat water. Add 8 drops of household bleach for every 1 gallon of water (or 2 drops of household bleach for every 1 litre of water) and wait 30 minutes before drinking.
• Store treated water in a clean, covered container.
2.
• Use safe water to brush your teeth, wash and prepare food.
• Clean food preparation areas and kitchen utensils with soap and safe water and dry completely before reuse
3.
4.
• Wash hands with soap and safe water after defecating.
• Defecate at least 30 meters (98 feet) away from any body of water and then bury faeces.
• Dispose of plastic bags containing faeces in latrines, at collection points if available, or bury it in the ground. Do not put plastic bags in chemical toilets.
• Dig new latrines or temporary pit toilets at least a half-metre (1.6 feet) deep and at least 30 metres (98 feet) away from any body of water.
5.
• Be sure to cook shellfish (like crabs and crayfish) until they are very hot all the way through.
*Avoid raw foods other than fruits and vegetables you have peeled yourself.
6.
• Wash yourself, your children, diapers/baby napkins, and clothes, 30 meters (98 feet) away from drinking water sources.
Implementing these preventive measures individually and collectively as a community is necessary for cholera outbreak prevention. These preventive messages should constitute the messages given to the general public at the community, LGA, State and national levels before and during an outbreak.
The Nigeria Centre for Disease Control (NCDC) continues to advocate for improved water, sanitation, hygiene as well as risk communications activities in States. Members of the public are advised to always seek care in a health facility if they have watery diarrhoea.
SUMMARY OF REPORTS
In the reporting week ending on June 3, 2018:
o There were 187 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has reinvigorated its efforts at eradicating Polio.
o 910 suspected cases of Cholera were reported from 16 LGAs in six States (Adawama – 423, Bauchi – 344, Borno – 20, Kano – 11, Plateau - 37 & Zamfara - 75). Of these, 12 were laboratory confirmed and six deaths were recorded.
o Five suspected cases of Lassa fever were reported in the reporting week. One was laboratory confirmed and no death was recorded.
o There were 27 suspected cases of Cerebrospinal Meningitis (CSM) reported from 18 LGAs in nine States (Borno – 1, Cross River – 1, Ebonyi – 2, Kaduna – 1, Katsina – 13, Nasarawa – 1, Ondo – 1, Taraba – 1, Yobe – 1 & Zamfara - 5). Of these, no was laboratory confirmed and two deaths were recorded.
o There were 306-suspected cases of Measles reported from 31 States. No laboratory-confirmed and no death was recorded.
In the reporting week, all States sent in their report except Delta State. Timeliness of reporting remains 89% in both the previous and current weeks (week 21 & 22) while completeness increases from 99% to 100% during the same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1. As at May 27th, 2018, no new case of WPV was recorded
1.2. In the reporting week, 127 cases of AFP were reported from 110 LGAs in 29 States & FCT
1.2.1. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
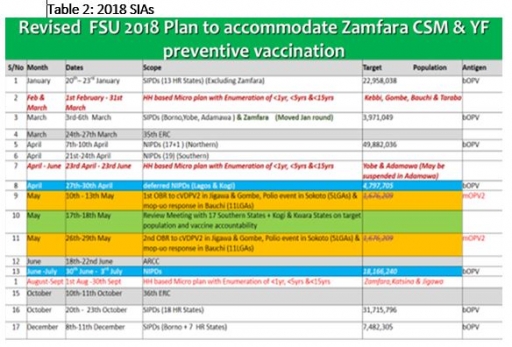
12.2 The 1st & 2nd Outbreak response (OBR) to cVDPV2 in Jigawa & Gombe States, Polio event in Sokoto (SLGAs) and mop-up response in 11 LGAs in Bauchi State conducted from 10th – 13th & 26th – 29th May 2018 using mOPV2 respectively
1.2.3 Two SIPDs and one NIPDs were conducted from January to April 2018 using bOPV in 18 high-risk States and 36 States plus FCT respectively
2. CEREBROSPINAL MENINGITIS (CSM)
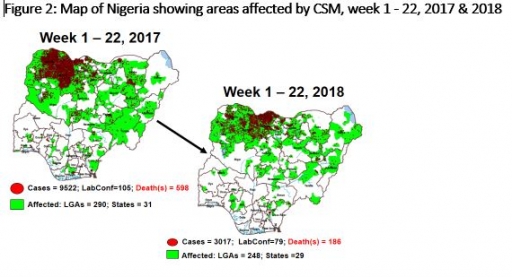
2.1 In the reporting week, 27 suspected Cerebrospinal Meningitis (CSM) cases and two deaths (CFR, 7.41%) were reported from 18 LGAs (ten States; Borno – 1, Cross River – 1, Ebonyi – 2, Kaduna – 1, Katsina – 13, Nasarawa – 1, Ondo – 1, Taraba – 1, Yobe – 1 & Zamfara - 5) compared with 42 suspected cases with one Lab. Confirmed and one death (CFR, 2.4%) from 22 LGAs (10 States) at the same period in 2017 (Figure 2)
2.2 Between weeks 1 and 22 (2018), 3017 suspected meningitis cases with 79 laboratory confirmed and 186 deaths (CFR, 6.17%) from 248 LGAs (29 States) were reported compared with 9570 suspected cases and 599 deaths (CFR, 6.26%) from 293 LGAs (31 States) during the same period in 2017.
2.3 Timeliness/completeness of CSM case-reporting from States to the National Level (2018 versus 2017): on average, 88.2% of the 26 endemic States sent CSM reports in a timely manner while 98.2% were complete in week 1 - 22, 2018 as against 76.4% timeliness and 92.3% completeness recorded within the same period in 2017
2.4 The 2018 CSM outbreak has been declared over following epidemiological review and decline in the number of cases
CHOLERA
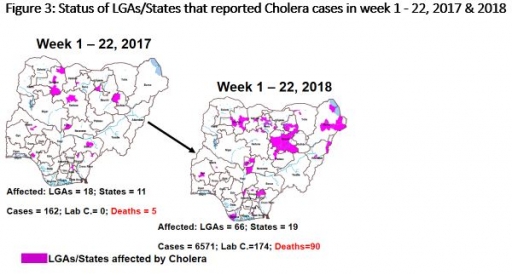
3.1 910 suspected cases of Cholera with 12 Laboratory Confirmed cases and six deaths (CFR, 0.66%) were reported from 16 LGAs (six States; Adawama – 423, Bauchi – 344, Borno – 20, Kano – 11, Plateau - 37 & Zamfara - 75) in week 22, 2018 compared with 77 suspected cases and one death (CFR, 1.3%) reported from four LGAs (two States) during the same period in 2017 (Figure 3)
3.2 Between weeks 1 and 22 (2018), 6571 suspected Cholera cases with 174 laboratory confirmed and 90 deaths (CFR, 1.37%) from 68 LGAs (19 States) were reported compared with 162 suspected cases and five deaths (CFR, 3.09%) from 18 LGAs (13 States) during the same period in 2017.
3.3 A National Emergency Operations Centre (EOC) for Cholera has been activated at level 2 at NCDC.
3.4 Rapid Response Teams have been deployed to respond to a recent cluster of cases in Kano, Bauchi, Plateau, Zamfara and Adamawa States.
3.5 National Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines available via http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
4.1 Five suspected cases of Lassa fever with one Laboratory confirmed were reported from two LGAs (two States) in week 22, 2018 compared with one suspected case reported from Abeokuta South LGA (Ogun State) at the same period in 2017
4.2 Laboratory results of the five suspected cases; one was positive for Lassa fever (Edo -1) while the remaining four were negative for Lassa fever & other VHFs (Ondo – 4)
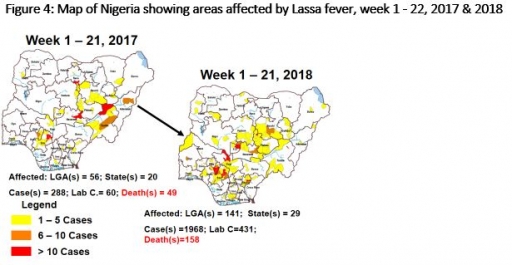
4.3 Between weeks 1 and 22 (2018), 1982 suspected Lassa fever cases with 432 laboratory confirmed cases and 118 deaths (CFR, 5.95%) from 141 LGAs (29 States) were reported compared with 288 suspected cases with 60 laboratory confirmed cases and 49 deaths (CFR, 16.78%) from 56 LGAs (20 States) during the same period in 2017 (Figure 4)
4.4 National VHF guidelines (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
4.5 NCDC and Irrua Specialist Teaching Hospital have conducted the first phase of nationwide training on Lassa fever case management in the South-West, South-East, South-South, North- East & North – West.
4 MEASLES
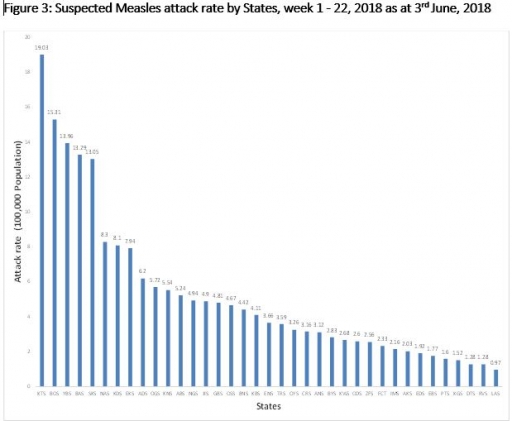
5.1 In the reporting week, 306 suspected cases of Measles were reported from 31 States compared with 361 suspected cases reported from 33 States during the same period in 2017
5.2 So far, 10688 suspected Measles cases with nine Lab. Confirmed and 94 deaths (CFR, 0.88 %) were reported from 36 States and FCT compared with 12094 suspected cases with 71 laboratory confirmed and 74 deaths (CFR, 0.61 %) from 37 States during the same period in 2017
5.3 Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 23, 2018
7.1. From week 1- 23, 149-suspected cases were reported, of which 140 were Influenza-like-illness (ILI), nine Severe Acute Respiratory Infection (SARI).
7.2 A total of 149 samples were received and 147 samples were processed. Of the processed samples, 138(93.9%) were ILI cases, nine (6.1%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 147 processed ILI samples, 16 (10.90%) was positive for Influenza A; 26(17.7%) positive for Influenza B and 105 (71.4%) were negative.
7.5 For the processed nine SARI samples, five (55.56%) were positive for Influenza A while the remaining four (44.44%) were negative.
7.6 42 (28.6%) of the processed 147 samples were positive for Influenza, with 16 (38.1%) of these positive for Influenza A and 26 (61.9%) positive for Influenza B.
7.5. The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for (0.0%), 11 (68.8%) and 5 (31.2%) of total influenza A positive samples respectively.
7.6 The subtypes B VICTORIA, B Not subtyped and B Yamagata account for 10(38.5%), 16(61.5%) and 0(0.0%) of the total influenza B positive samples respectively
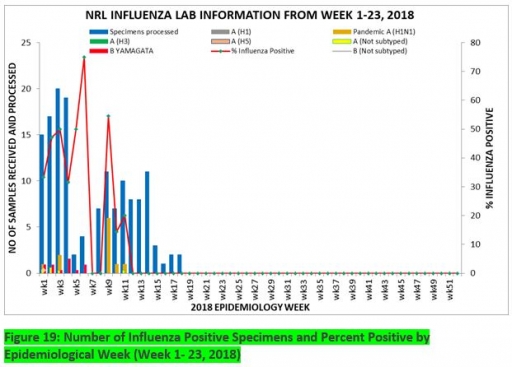
7.7 The percentage of influenza-positive was highest (75.0%) in week 6, 2018
7.8 In the reporting week 1 -23, two samples were left unprocessed
Figure 19: Number of Influenza Positive Specimens and Percent Positive by Epidemiological Week (Week 1- 23, 2018)
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
