In the last two years, Nigeria has experienced outbreaks of Lassa fever, Monkeypox, Cerebrospinal meningitis, cholera and a resurgence of yellow fever. During some of these outbreaks notably of Lassa fever, there have been reports of health care worker infections.
This has further highlighted the need for health care workers to adhere strictly to infection prevention and control (IPC) practices to keep themselves and their patients safe.
IPC is a universally relevant component of all health systems and promotes the health and safety of both people who use services and those who provide them. Effective IPC is a key determinant of the quality of health service delivery to achieve people-centered, integrated universal health coverage (World Health Organization, 2016).
The Nigeria Centre for Disease Control in delivering its mandate to protect the health of Nigerians, is collaborating with the Robert Koch institute of Germany, Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ)in the ‘MAURICE’ IPC Project. This project aims at prevention of healthcare acquired infections among health care workers in Nigeria.
This is coordinated by NCDC and a technical working group comprising of national IPC stakeholders with the primary objective to develop a harmonised national IPC manual for all personnel working in health care setting. In addition, the project supports a ‘training of trainers’ workshop for frontline health care workers as ‘IPC change agents’ using the participatory quality development approach (PQDA). In addition, quick reference IPC documents “one pagers and miniatures†(pocket hand book) on standard and transmission based precautions have been developed.
The IPC PQDA workshop was piloted in FCT university of Abuja teaching hospital and is currently being implemented in Lagos state where 28 health care workers from seven private and seven public facilities were trained as IPC change agents.
The PQDA model employs the “bottom top approach†which promotes ownership by staff in a health care institution and leadership engagement for an IPC enabling environment with consequent sustainability of an IPC culture.
The achievements of the PQDA from the pilot and Lagos workshops have been remarkable with impressive feedback from both participants and the medical directors of the participating health facilities.
The significant improvement of infection prevention and control measures in the country will require a scale-up of the project across all states. The last phase of the project is currently ongoing and involves an operational research for the adequate step by step documentation of all the processes of the project implementation.
In a country like Nigeria where there is a high burden of infectious diseases, the responsibility should not be left to the government or health care workers alone to prevent infectious diseases. Adopting standard IPC measures such as a good hand hygiene into our daily routine can reduce deaths due to diarrheal diseases (e.g. cholera) by half, the risk of respiratory infections by 16% and prevent up to a million deaths annually. It is our collective responsibility to ensure a safer Nigeria through standard infection prevention and control.
By raising IPC Change Agents through the MAURICE Project, we are leading the change to create a healthier and safer Nigeria through the prevention and control of diseases of public health importance and strengthening our national health security.
SUMMARY OF REPORTS
In the reporting week ending on June 17, 2018:
o There were 116 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has reinvigorated its efforts at eradicating Polio.
o 725 suspected cases of Cholera were reported from 19 LGAs in eight States (Adamawa – 80, Bauchi – 323, Borno – 2, Kaduna – 1, Kano – 42, Kogi – 20, Plateau - 19 & Zamfara - 238). Of these, nine were laboratory confirmed and nine deaths were recorded.
o Six suspected cases of Lassa fever were reported from three LGAs in two States (Katsina – 1 & Ondo – 5) this reporting week. One was laboratory confirmed and no death was recorded.
o There were 19 suspected cases of Cerebrospinal Meningitis (CSM) reported from ten LGAs in four States (Kano – 1, Katsina – 12, Sokoto – 1 & Yobe - 5). Of these, no was laboratory confirmed and no death was recorded.
o There were 188-suspected cases of Measles reported from 28 States. No laboratory-confirmed and no death was recorded.
In the reporting week, all States sent in their report except Akwa-Ibom, Cross River, Delta and Imo States. Timeliness of reporting remains 89% in both the previous and current weeks (week 23 & 24) while completeness decreased from 100% to 99% during the same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1. As at June 17th, 2018, no new case of WPV was recorded
1.2. In the reporting week, 116 cases of AFP were reported from 101 LGAs in 29 States & FCT
1.2.1. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
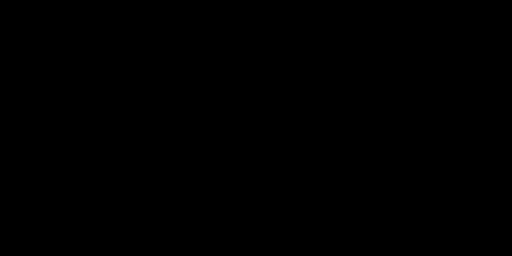
1.2.2. NIPDs is ongoing from 30th June to 3rd July 2018 using bOPV in 36 States plus FCT
12.2 The 1st & 2nd Outbreak response (OBR) to cVDPV2 in Jigawa & Gombe States, Polio event in Sokoto (SLGAs) and mop-up response in 11 LGAs in Bauchi State conducted from 10th – 13th & 26th – 29th May 2018 using mOPV2 respectively
1.2.3 Two SIPDs and one NIPDs were conducted from January to April 2018 using bOPV in 18 high-risk States and 36 States plus FCT respectively
2. CEREBROSPINAL MENINGITIS (CSM)
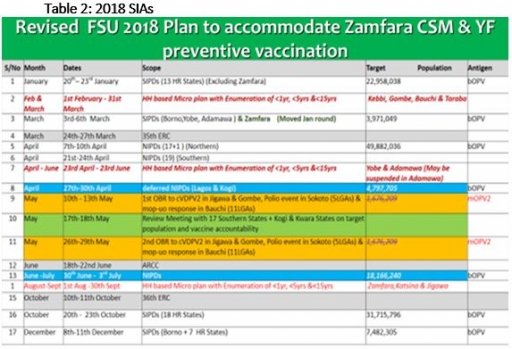
2.1 In the reporting week, 19 suspected Cerebrospinal Meningitis (CSM) cases were reported from ten LGAs (four States; Kano – 1, Katsina – 12, Sokoto – 1 & Yobe - 5) compared with 41 suspected cases and one death (CFR, 2.4%) from 20 LGAs (seven States) at the same period in 2017 (Figure 2)
2.2 Between weeks 1 and 22 (2018), 3167 suspected meningitis cases with 100 laboratory confirmed and 206 deaths (CFR, 6.50%) from 248 LGAs (29 States) were reported compared with 9656 suspected cases and 601 deaths (CFR, 6.22%) from 296 LGAs (31 States) during the same period in 2017.
2.3 Timeliness/completeness of CSM case-reporting from States to the National Level (2018 versus 2017): on average, 88.2% of the 26 endemic States sent CSM reports in a timely manner while 98.2% were complete in week 1 - 24, 2018 as against 76.4% timeliness and 92.3% completeness recorded within the same period in 2017
2.4 The 2018 CSM outbreak has been declared over following epidemiological review and decline in the number of cases
CHOLERA
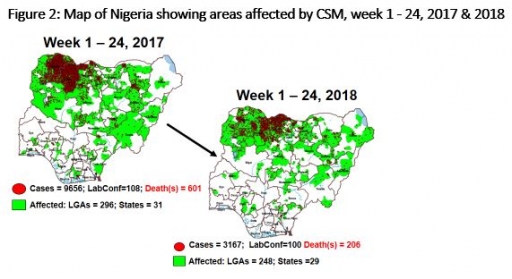
3.1 725 suspected cases of Cholera with nine Laboratory Confirmed cases and nine deaths (CFR, 1.24%) were reported from 19 LGAs (eight States; Adawama – 80, Bauchi – 323, Borno – 2, Kaduna – 1, Kano – 42, Kogi – 20, Plateau - 19 & Zamfara - 238) in week 24, 2018 compared with 108 suspected cases with eight Laboratory confirmed were reported from seven LGAs (three States) during the same period in 2017 (Figure 3)
3.2 Between weeks 1 and 24 (2018), 8294 suspected Cholera cases with 217 laboratory confirmed and 109 deaths (CFR, 1.31%) from 71 LGAs (19 States) were reported compared with 396 suspected cases and six deaths (CFR, 1.52%) from 21 LGAs (13 States) during the same period in 2017.
3.3 A National Emergency Operations Centre (EOC) for Cholera has been activated at level 2 at NCDC.
3.4 Rapid Response Teams have been deployed to respond to the recent cluster of cases in Kano, Bauchi, Plateau, Zamfara and Adamawa States.
3.5 National Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines available via http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
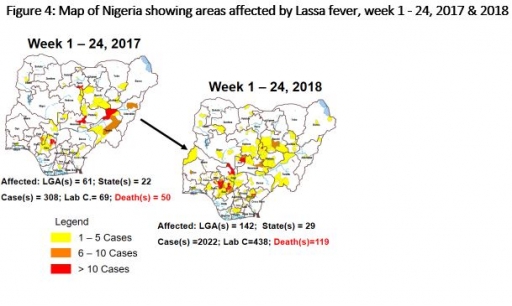
4.1 Six suspected cases of Lassa fever with one Laboratory confirmed were reported from three LGAs (two States) in week 24, 2018 compared with six suspected cases with three Laboratory confirmed and one death (CFR, 16.7%) reported from four LGAs (three States) at the same period in 2017
4.2 Laboratory results of the six suspected cases; one was positive for Lassa fever (Ondo -1) while the remaining five were negative for Lassa fever & other VHFs (Katsina – 1 & Ondo - 5)
4.3 Between weeks 1 and 24 (2018), 2022 suspected Lassa fever cases with 438 laboratory confirmed cases and 119 deaths (CFR, 5.89%) from 141 LGAs (29 States) were reported compared with 308 suspected cases with 68 laboratory confirmed cases and 50 deaths (CFR, 16.23%) from 61 LGAs (22 States) during the same period in 2017 (Figure 4)
4.4 National VHF guidelines (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
4.5 Irrua Specialist Teaching Hospital (ISTH) in collaboration with NCDC has completed the first phase of National Intensive Clinical Workshop on Diagnosis and Management of Lassa fever in the six geopolitical zones. The participants were State Epidemiologist, State DSNO, State Lab focal person, State health educator, case management physician and Nurse from all the 36 States & FCT.
4.6 The 2nd phase of the training was a practical hands-on session for the case management Physicians, Nurses, and State Lab. Focal persons at ISTH. Other participants included the Lab focal person at the National reference laboratories where Lassa fever is carried out. The hands-on session was carried out for two days (28th – 29th June 2018). Participants were involved in the management of Lassa fever patients in the hospital and the Lab focal persons were engaged in carrying out testing of Lassa fever samples
5 MEASLES
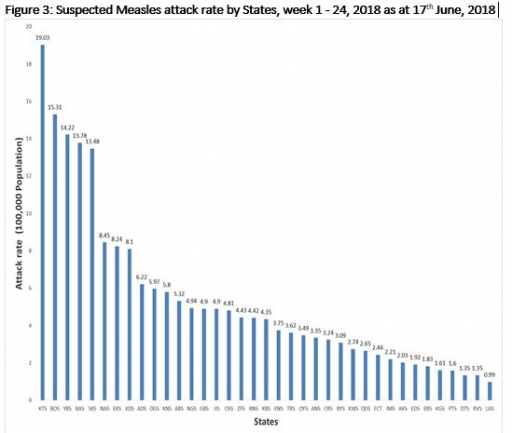
5.1 In the reporting week, 188 suspected cases of Measles were reported from 28 States compared with 579 suspected cases with Laboratory confirmed and two deaths (CFR, 0.35%) reported from 35 States during the same period in 2017
5.2 So far, 11256 suspected Measles cases with 13 Lab. Confirmed and 94 deaths (CFR, 0.84 %) were reported from 36 States and FCT compared with 13144 suspected cases with 77 laboratory confirmed and 76 deaths (CFR, 0.58 %) from 37 States during the same period in 2017
5.3 Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management
6 Yellow fever
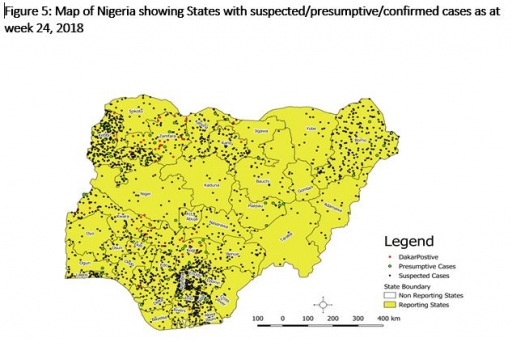
6.1 In this reporting week 11th June – 17th June 2018, 88 suspected cases were reported from Gombe Specialist Hospital, NCDC’s Central Public Health Laboratory (CPHL) Lagos and Maitama District Hospital (MDH) Abuja Laboratories and Kebbi State YF surveillance line list
6.2 No new in-country presumptive positives in the reporting week, last presumptive positive case in the Nigerian lab was 10-May-18 and last IP Dakar confirmed case from Nigeria was on 6-June -2018
6.3 From the onset of this outbreak on September 12, 2017, a total of 2,074 suspected yellow fever cases with 47 Laboratory confirmed and 47 deaths (CFR, 2.3%) were reported from 460 LGAs (36 States & FCT)
6.4 Predominant age groups affected among the suspected cases are 20 years and below accounting for 62.3%; [male to female ratio is 1.4 to 1 (male 58.2%, female 41.8%)]
6.5 Surveillance has been intensified across states by NCDC
6.6 NCDC had provided onsite support to Kwara, Kogi, Plateau, Kebbi, Kano and Katsina States
6.7 Entomological survey, conducted in Kwara, Zamfara, Kebbi, Kano and Katsina States Surveillance and laboratory data harmonization and updating is on-going
6.8 Developed the chronogram of events for the phase 2 PMVC and strategies to
6.9 NCDC and partners had completed an assessment of some laboratories in Nigeria for possible inclusion into the testing laboratory network
6.10 Media monitoring on traditional and new media channels and sharing YF messages on social media.
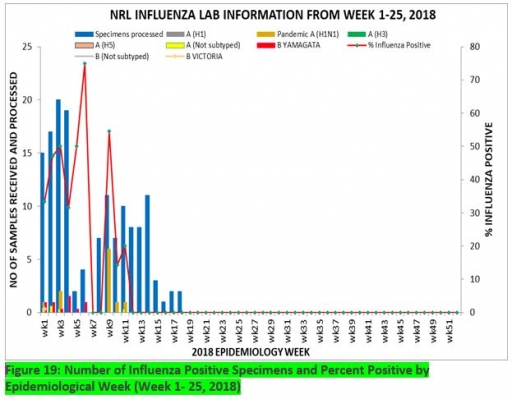
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 25, 2018
7.1. From week 1- 25, 152-suspected cases were reported, of which 143 were Influenza-like-illness (ILI), nine Severe Acute Respiratory Infection (SARI).
7.2 A total of 152 samples were received and 147 samples were processed. Of the processed samples, 138(93.9%) were ILI cases, nine (6.1%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 147 processed ILI samples, 16 (10.90%) was positive for Influenza A; 26(17.7%) positive for Influenza B and 105 (71.4%) were negative.
7.5 For the processed nine SARI samples, five (55.56%) were positive for Influenza A while the remaining four (44.44%) were negative.
7.6 42 (28.6%) of the processed 147 samples were positive for Influenza, with 16 (38.1%) of these positive for Influenza A and 26 (61.9%) positive for Influenza B.
7.5. The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for (0.0%), 11 (68.8%) and 5 (31.2%) of total influenza A positive samples respectively.
7.6 The subtypes B VICTORIA, B Not subtyped and B Yamagata account for 10(38.5%), 16(61.5%) and 0(0.0%) of the total influenza B positive samples respectively
7.7 The percentage of influenza-positive was highest (75.0%) in week 6, 2018
7.8 In the reporting week 1 -25, five samples were left unprocessed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
