The Lassa fever outbreak continued in Epi-week 3 with 107 suspected cases, 53 confirmed cases reported from seven States. 14 deaths have been recorded in confirmed and probable cases, giving a case fatality rate (CFR) of 25%. As at the end of epi week 3, ten healthcare workers had been affected.
It is important to note that in providing care for confirmed cases, the Lassa fever guidelines should be adhered to, for compliance with provision of the acceptable standard of care for all cases. All health care workers are advised to use universal precautions at all times. Suspected cases who show classic symptoms of Lassa fever and are awaiting laboratory confirmation should have treatment commenced pending the outcome of laboratory investigations. Lassa fever testing is not indicated for contacts, unless there are symptoms of Lassa fever.
Identification of contacts is very critical in breaking transmission and preventing spread of Lassa fever in the community. A contact is a person who has been exposed to an infected person or to an infected person’s secretions, excretions, or tissues within three weeks of the patient’s illness. On identification, contacts are categorized based on the degree of exposure to a confirmed case to no-risk, low-risk and high-risk.
No direct contact with the patient or body fluids.
• Casual contact, e.g. sharing a room with the patient, without direct contact with body fluids or other potentially infectious material.
Direct contact with the patient, e.g. routine medical/nursing care, OR
Unprotected exposure of skin or mucous membranes to potentially infectious blood or body fluids, including clothing and bedding.
• This includes unprotected handling of clinical/laboratory specimens; mucosal exposure to splashes; needle-stick injury and kissing and/or sexual contact.
Only high-risk contacts can be provided with treatment. Other contacts are monitored closely for 21 days for any symptoms suggestive of Lassa fever.
The National Lassa Fever Emergency Operations Centre (LF-EOC) has been activated to coordinate the response to this outbreak, in collaboration with partner agencies. As part of the response activities, the Nigeria Centre for Disease Control (NCDC) through the LF-EOC has distributed drugs, Personal Protective Equipment (PPEs) and other consumables to affected states for management of confirmed cases and contacts. More information on the outbreak and the guidelines for Lassa fever can be accessed on the NCDC website: www.ncdc.gov.ng
SUMMARY OF REPORTS
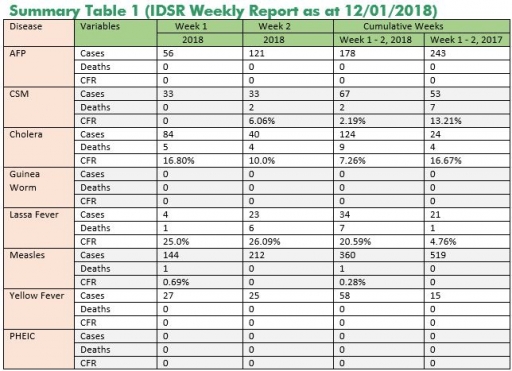
In the reporting week ending on January 12, 2018:
o There were 121 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has reinvigorated its efforts at eradicating Polio.
o 40 suspected cases of Cholera were reported from 11 LGAs in three States (Bauchi – 3, Kaduna – 6 & Kano – 31). Of these, no was laboratory confirmed and four deaths were recorded.
o 23 suspected cases of Lassa fever were reported from eight LGAs in six States (Anambra – 1, Bauchi – 2, Ebonyi – 7, Edo – 3, Nasarawa – 1 & Ondo - 9). 12 were laboratory confirmed and six deaths were recorded.
o There were 33-suspected cases of Cerebrospinal Meningitis (CSM) reported from 22 LGAs in nine States (Abia – 1, Bauchi – 2, Borno -1, Ebonyi – 1, Edo – 2, FCT -1, Katsina - 13, Kebbi – 2, Sokoto – 4, Yobe - 6 & Zamfara – 15). Of these, seven were laboratory confirmed and two deaths were recorded. Ongoing surveillance for CSM has been intensified in all the 26 States in the Nigeria meningitis belt and case-based surveillance commenced from 4th December 2017.
o There were 212- suspected cases of Measles reported from 33 States. None was laboratory confirmed and no death was recorded.
In the reporting week, all States sent in their report. This is a remarkable improvement! Timeliness of reporting is 86% in both previous and current weeks (Week 52, 2017 and Week 1, 2018) while completeness is 100% and 89% at the same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1. As at January 14th, 2018, no new case of WPV was recorded
1.2. In the reporting week, 121 cases of AFP were reported from 111 LGAs in 20 States & FCT
1.2.1. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
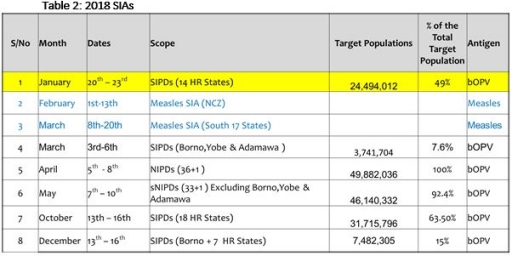
1.2.2. The 1st round of SIPDs in 2018 conducted from 20th – 23rd January 2018 in the 14 high-risk States using bOPV. The schedule for other SIAs is as described in Table 2
1.3. Six confirmed WPVs were isolated in 2014.
1.4. The SIAs were strengthened with the following events:
1.4.1. Immunisation for all vaccine-preventable diseases in some selected wards/LGAs.
1.4.2. Use of health camp facilities.
1.4.3. Field supportive supervision and monitoring.
1.4.4. Improved Enhanced Independent Monitoring (EIM) and Lots Quality Assessments (LQAs) in all Polio high-risk States.
1.4.5. High level of accountability framework
2. CEREBROSPINAL MENINGITIS (CSM)
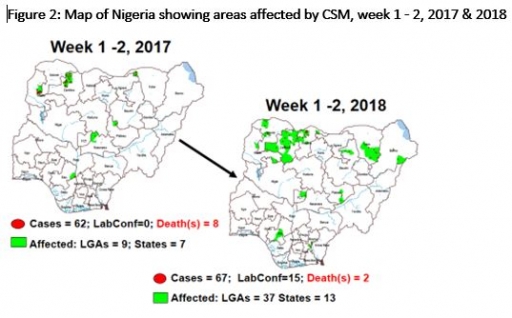
2.1 In the reporting week 1 (1 or 2?), 33 suspected Cerebrospinal Meningitis (CSM) cases with eight Laboratory confirmed were reported from 20 LGAs (six States; Ebonyi (how many?), FCT – 1, Katsina - 9, Plateau – 2, Sokoto – 4 & Zamfara - 15) compared with 33 suspected cases and three deaths (CFR, 9.1%) from three LGAs (three States) at the same period in 2017 (Figure 2)
2.2 Between weeks 1 and 2 (2018), 67 suspected Cholera cases with 15 laboratory confirmed and two deaths (CFR, 2.19%) from 37 LGAs (13 States) were reported compared with 24 suspected cases and four deaths (CFR, 16.67%) from 3 LGAs (three States) during the same period in 2017. (Cholera???)
2.3 Timeliness/completeness of CSM case-reporting from States to the National Level (2017 versus 2016): on average, 88.5% of the 26 endemic States sent CSM reports in a timely manner while 88.5% were complete in week 1 - 2, 2018 as against 76.9% timeliness and 78.8% completeness recorded within the same period in 2017
2.4 The National CSM Emergency Operations Centre has been activated and is currently in response mode
2.5 Enhanced surveillance/ case-based surveillance began 1st of December 2017
2.6 Rapid Response Teams currently deployed to support response in Zamfara and Katsina States
2.7 The National CSM Guidelines have been finalised and available via http://ncdc.gov.ng/themes/common/docs/protocols/51_1510449270.pdf
2.8 State CSM Emergency Operations Centre has been activated in Zamfara, Katsina and Sokoto States respectively
CHOLERA
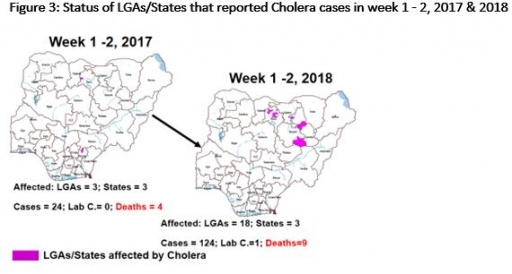
2.9 40 suspected cases of Cholera and four deaths (CFR, 10.0%) were reported from 11 LGAs (three States: Bauchi – 3, Kaduna – 6 & Kano - 31) in week 2 compared with 24 cases and four deaths (CFR, 16.67%) reported from three LGAs (three States) during the same period in 2017 (Figure 3).
2.10 Between weeks 1 and 2 (2018), 67 suspected Cholera cases with 15 laboratory confirmed and two deaths (CFR, 2.19%) from 37 LGAs (13 States) were reported compared with 24 suspected cases and four deaths (CFR, 16.67%) from 3 LGAs (three States) during the same period in 2017.
2.11 National Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines have been finalised: http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
2.12 States are enjoined to intensify surveillance, implement WASH activities and ensure early reporting.
LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
4.1 23 suspected cases of Lassa fever with 12 Laboratory confirmed and six deaths (CFR, 26.1%) were reported from eight LGAs (six States: Anambra – 1, Bauchi – 2, Ebonyi – 7, Edo – 3, Nasarawa – 1 & Ondo - 9) in week 2, 2018 compared with 14 suspected cases with four Lab. Confirmed and one death (CFR, 7.1%) reported from five LGAs (five States) at the same period in 2017
4.2 Laboratory results of the 23 suspected cases; 12 positive for Lassa fever (Anambra – 1, Ebonyi – 7, Edo – 3 & Ondo - 1), 11 were negative for Lassa fever & other VHFs (Bauchi – 2, Nasarawa – 1 & Ondo - 8)
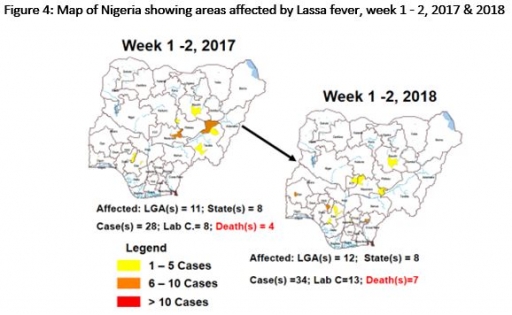
4.3 Between weeks 1 and 2 (2018), 34 suspected Lassa fever cases with 13 laboratory confirmed cases and 7 deaths (CFR, 20.59%) from 12 LGAs (eight States) were reported compared with 28 suspected cases with five laboratory confirmed cases and four deaths (CFR, 14.29%) from 11 LGAs (eight States) during the same period in 2017 (Figure 4)
4.4 Investigation and active case search ongoing in affected States with coordination of response activities by the NCDC with support from partners
4.5 National Lassa Fever Working Group has been escalated to National Emergency Operations Centre on the 22nd January, 2018
4.6 Response materials for VHF provided to support States and health facilities
4.7 National VHF guidelines (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
4.8 VHF case-based forms completed by affected States are being entered into the new VHF management system. This system allows for the creation of a VHF database for the country. Data from the VHF database is currently being analysed to inform decision making in the coming year
4.9 Onsite support ongoing in Ebonyi and Ondo States by the NCDC and partners
4.10 Offsite support provided by NCDC/partners in all affected States
4.11 States are enjoined to intensify surveillance and promote Infection, Prevention and Control (IPC) measures in health facilities
5 MEASLES
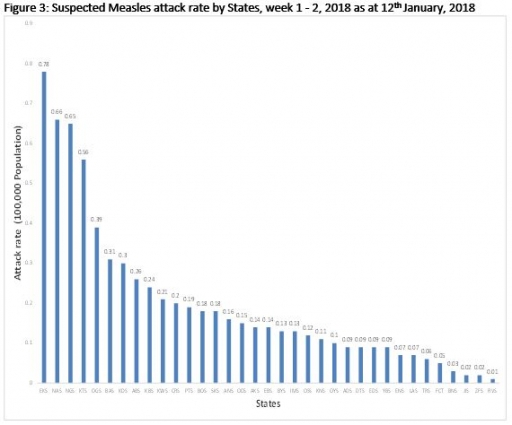
5.1 In the reporting week, 212 suspected cases of Measles were reported from 33 States compared with 288 suspected cases reported from 24 States during the same period in 2017
5.2 So far, 360 suspected Measles cases and one death (CFR, 0.28%) were reported from 34 States and FCT compared with 519 suspected cases with two laboratory-confirmed during the same period in 2017
5.3 Response measures include immunisation for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management
5.4 Measles mass campaign conducted in seven North West and North East States from 9th – 14th November 2017 and 30th November – 5th December 2017 respectively.
5.5 Proposed Measles mass campaign for North Central and Southern States scheduled for February 1 - 13 and March 8 – 20, 2018 respectively.
6 GUINEA WORM DISEASE
6.1 In the reporting week, no rumour report of Guinea Worm disease was received from any State.
6.2 Nigeria has celebrated eight consecutive years of zero reporting of Guinea worm disease in the country. The Country has been officially certified free of Dracunculiasis transmission by the International Commission for the Certification of Dracunculiasis Eradication (ICCDE).
(For further information, contact Nigeria Guinea Worm Eradication Program / Neglected Tropical Diseases Division, Public Health Department/Federal Ministry of Health)
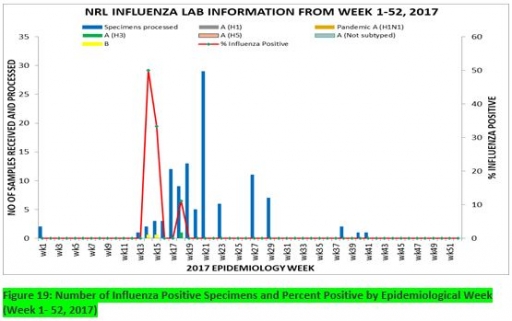
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 52, 2017
7.1. From week 1-52, 150-suspected cases were reported, of which 148 were Influenza-like-illness (ILI), eight Severe Acute Respiratory Infection (SARI).
7.2 150 samples were received of which 107 were processed. Of the processed samples, 99(92.5%) were ILI cases, eight (7.5%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 99 processed ILI samples, 1(1.01%) was positive for Influenza A; two (2.02%) positive for Influenza B and 96(96.97%) were negative.
7.5. Of the eight processed SARI samples, none was positive for Influenza A and Influenza B.
7.6. Three (2.80%) of the processed 107 samples were positive for Influenza, with one (33.3%) of these positive for Influenza A and two (66.7%) positive for Influenza B.
7.7. The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for (100%), 0 (0.0%) and 0 (0.0%) of total influenza A positive samples respectively.
7.8. The percentage influenza positive was highest (50.0%) in week 14, 2017
7.9. In the reporting week 50, none samples were left unprocessed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
