The seamless flow of information through an effective surveillance system is very important for the early detection and response to outbreaks. In addition, it enables feedback that helps to improve the efficiency and effectiveness of health programs, and improve health.
Given the need for a more competent informatics workforce in Nigeria, the Nigeria Centre for Disease Control (NCDC) in collaboration with the US Centers for Disease Control (US CDC) and Chinese Centre for Disease Control has begun the Growing Expertise in E-Health Knowledge and Skills (GEEKS) training in Abuja, Nigeria.
GEEKS is a three-tier approach to develop and maintain informatics capacity within a country’s health system through the development of a centre of excellence for informatics training. As a program hosted by Nigeria’s National Public Health Institute, GEEKS is a valuable, cross-cutting program to strengthen and improve health systems, population health, and global health security in Nigeria and Africa. The key target beneficiaries of the GEEKS Program include frontline public health workers, public health leaders, and informatics scientists and practitioners.
The first workshop in Nigeria was held in Abuja from 24th to 28th September, 2018. This workshop was the first tier of the GEEKS program with participants drawn from the Departments/programs of the Federal Ministry of Health, National Primary Healthcare Development Agency, Federal Ministry of Agriculture & Rural Development, State Ministries of Health (State Director of Public health, State Epidemiologist & State DSNOs), AIDS Prevention Initiative Nigeria (APIN), Institute of Human Virology, Nigeria (IHVN), Catholic Caritas Foundation of Nigeria (CCFN), Centre for Integrated Health Programme (CIHP), US-CDC, AFENET, Pro-Health, University of Maryland Baltimore, E-Health Nigeria and other stakeholders. Candidates who are successful at this level will proceed to the second tier.
The GEEKS program is an important strategy to strengthen surveillance and health information systems in Nigeria.
SUMMARY OF REPORTS
In the reporting week ending on September 16, 2018:
o There were 157 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as polio. The last reported case of polio in Nigeria was in August 2016. Active case search for AFP is being intensified with the goal to eliminate polio in Nigeria.
o There were 2126 suspected cases of Cholera reported from 52 LGAs in 13 States (Adamawa – 69, Bauchi – 3, Borno – 281, Ebonyi – 1, Gombe – 94, Kaduna – 3, Kano – 110, Katsina – 263, Kwara – 6, Lagos – 3, Osun – 1, Yobe - 252 and Zamfara - 1040). Of these, 27 were laboratory confirmed and 38 deaths were recorded.
o Seven suspected cases of Lassa fever were reported from six LGAs in five States (Abia -1, Bauchi – 1, Delta – 1, Edo – 2 & Enugu - 2). Two were laboratory confirmed and no death was recorded.
o There were 25 suspected cases of Cerebrospinal Meningitis (CSM) reported from 15 LGAs in nine States (Cross River – 2, Delta – 3, Ebonyi – 3, Enugu – 5, Imo – 5, Kano – 1, Katsina – 2, Ondo – 1 & Yobe – 3). Of these, none was laboratory confirmed and no death was recorded.
o There were 171 suspected cases of measles reported from 31 States. None was laboratory confirmed and no death was recorded.
In the reporting week, all States sent in their report except Jigawa and Taraba States. Timeliness of reporting remains 87% in both previous and current weeks (36 & 37) while completeness also remains 99% at same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1. As at September 16th 2018, no new case of WPV was recorded
1.2. In the reporting week, 157 cases of AFP were reported from 137 LGAs in 34 States
1.3. Between week 1 and 37 2018, 6095 suspected cases of AFP have been reported from 743 LGAs in 37 States
1.3.1. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
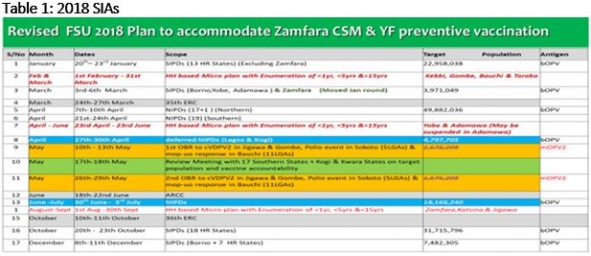
1.3.2. The 2nd NIPDs was conducted from 30th June to 3rd July, 2018 using bOPV in 36 States plus FCT
1.3.3. The 1st & 2nd Outbreak response (OBR) to cVDPV2 in Jigawa & Gombe States, Polio event in Sokoto (SLGAs) and mop-up response in 11 LGAs in Bauchi State conducted from 10th – 13th & 26th – 29th May, 2018 using mOPV2 respectively
1.3.4. Two SIPDs and one NIPDs were conducted from January to April, 2018 using bOPV in 18 high risk States and 36 States plus FCT respectively
2. CEREBROSPINAL MENINGITIS (CSM)
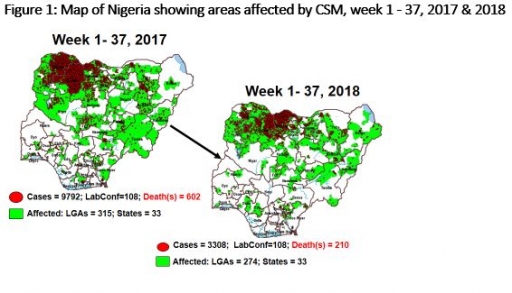
2.1 In the reporting week, 25 suspected Cerebrospinal Meningitis (CSM) cases were reported from 15 LGAs (nine States; Cross River – 2, Delta – 3, Ebonyi – 3, Enugu – 5, Imo – 5, Kano – 1, Katsina – 2, Ondo – 1 & Yobe – 3) compared with two suspected cases reported from two LGAs (two States) at the same period in 2017 (Figure 1)
2.2 Between weeks 1 and 37 (2018), 3308 suspected meningitis cases with 108 laboratory confirmed and 210 deaths (CFR, 6.4%) from 274 LGAs (33 States) were reported compared with 9792 suspected cases and 602 deaths (CFR, 6.2%) from 315 LGAs (33 States) during the same period in 2017.
2.3 Timeliness/completeness of CSM case-reporting from States to the National Level (2018 versus 2017): on average, 88.2% of the 26 endemic States sent CSM reports in a timely manner while 98.2% were complete in week 1 - 37, 2018 as against 76.4% timeliness and 92.3% completeness recorded within the same period in 2017
CHOLERA
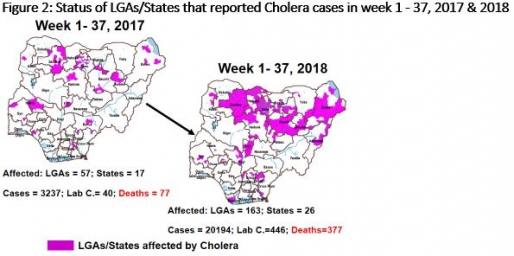
3.1 2126 suspected cases of Cholera with ten Lab. Confirmed and 58 deaths (CFR, 2.73%) were reported from 52 LGAs (13 States; Adamawa – 69, Bauchi – 3, Borno – 281, Ebonyi – 1, Gombe – 94, Kaduna – 3, Kano – 110, Katsina – 263, Kwara – 6, Lagos – 3, Osun – 1, Yobe - 252 and Zamfara - 1040) in week 37, 2018 compared with 907 suspected cases with one Lab. Confirmed and 26 deaths (CFR, 2.9%) reported from eight LGAs (six States) during the same period in 2017 (Figure 2).
3.2 Between weeks 1 and 37 (2018), 20,194 suspected Cholera cases with 446 laboratory confirmed and 377 deaths (CFR, 1.9%) from 163 LGAs (26 States) were reported compared with 3237 suspected cases and 77 deaths (CFR, 2.4%) from 57 LGAs (17 States) during the same period in 2017.
3.3 A National Emergency Operations Centre (EOC) for Cholera has been activated at level 2 at NCDC.
3.4 Rapid Response Teams have been deployed to respond to recent cluster of cases in Kano, Bauchi, Plateau, Zamfara, Adamawa and Katsina States.
3.5 NCDC and partners conducted the development of medium term strategies for Cholera control including mapping of the hot spots in Nigeria on the 19th of July, 2018.
3.6 A National coordination team led by the NCDC Incident Manager conducted an advocacy visit to Sokoto and Zamfara States to reinforce the ongoing response, strengthen the IMS structure and partner collaboration.
3.7 National Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines available via http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
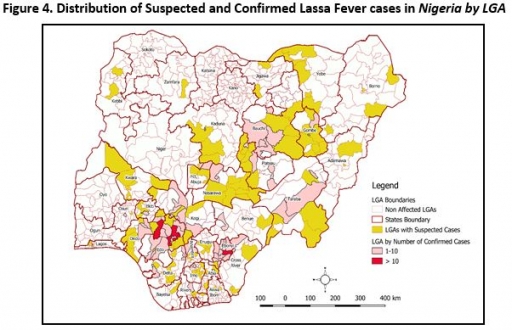
LASSA FEVER
4.1 In the reporting Week 37 (10 – 16 September, 2018) tw new confirmed I cases were reported from Edo State with no new death recorded.
4.2 From 1st January to 16th September 2018, a total of 2559 suspectedi cases have been reported from 22 states. Of these, 506 were confirmed positive, 10 are probable, 2044 negative (not a case)
4.3 Since the onset of the 2018 outbreak, there have been 133 deaths in confirmed cases and 10 in probable cases. Case Fatality Rate in confirmed cases is 26.3%
4.4 22 states have recorded at least one confirmed case across 88 Local Government Areas (Edo, Ondo, Bauchi, Nasarawa, Ebonyi, Anambra, Benue, Kogi, Imo, Plateau, Lagos, Taraba, Delta, Osun, Rivers, FCT, Gombe, Ekiti, Kaduna, Abia, Adamawa and Enugu). Twenty states have exited the active phase of the outbreak while two – Edo and Delta States remain activeiv
4.5 NCDC and Partners deployed Rapid Response Team (RRT) to Enugu and Edo States
4.6 Supplies for Lassa fever management procured through UNICEF and distributed to all LF affected states
4.7 Lassa fever international Conference registration, abstract submission and sponsorship now open to the public on the conference website www.lic.ncdc.gov.ng
4.8 The Lassa fever national multi-partner, multi-agency Technical Working Group (TWG) continues to coordinate response activities at all levels. Response and laboratory supplies have been provided to priority States
4.9 National VHF guidelines (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) are available on the NCDC website
4.10 http://ncdc.gov.ng/diseases/guidelines
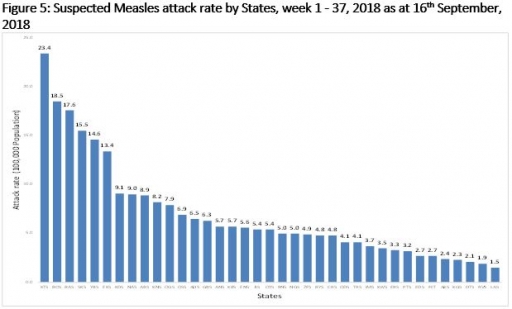
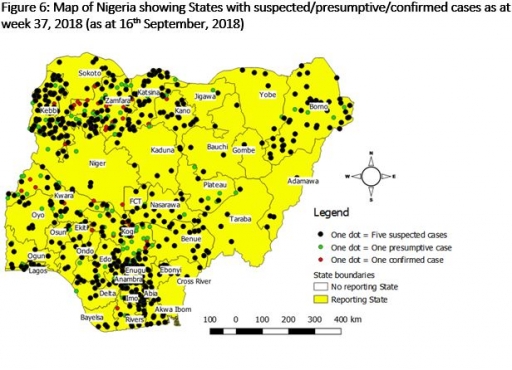
5 MEASLES
5.1 In the reporting week, 171 suspected cases of Measles were reported from 31 States compared with 209 suspected cases reported from 29 States during the same period in 2017
5.2 So far, 14066 suspected Measles cases with 901 Lab. Confirmed and 100 deaths (CFR, 0.71%) were reported from 36 States and FCT compared with 17772 suspected cases with 108 laboratory confirmed and 105 deaths (CFR, 0.56 %) from 37 States during the same period in 2017
5.3 Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management
5.4 NCDC and partners visited Edo and Cross River states to assess the laboratories in preparation for the establishment of a Zonal Measles/YF lab in the South South States
5.5 NCDC RRT conducted detailed investigation of measles outbreak in Oyo State
6 Yellow fever
6.1 In this reporting week 10th – 16th September, 2018, 178 suspected cases were added to the national line list
6.2 Six new in-country presumptive positive cases and one inconclusive case were reported in the reporting week from two diagnostic laboratories and last IP Dakar confirmed case from Nigeria was on 6th June, 2018
6.3 From the onset of this outbreak on September 12, 2017, a total of 3,015 suspected yellow fever cases with 47 Laboratory confirmed and 51 deaths (CFR, 1.7%) have been reported from 543 LGAs (36 States & FCT)
6.4 Predominant age groups affected among the suspected cases are 20 years and below accounting for 57.4%; [male to female ratio is 1.4 to 1 (male 57.5%, female 42.5%)]
6.5 Yellow fever reactive vaccination campaigns conducted in the following States [Kebbi (7 LGAs), Niger (5 LGAs), Sokoto (1 LGA) & Katsina (1 LGA)]
6.6 Yellow fever vaccination campaigns have been successfully completed in six States (Nassarawa, Cross River, Akwa-Ibom, Kogi, Kwara & Zamfara) and 57 political wards in 25 LGAs in Borno State
6.7 Surveillance activities have been intensified across all States
6.8 NCDC and partners have completed the assessment of some laboratories in Nigeria for possible inclusion into the testing laboratory network
6.9 NCDC & partners conducted detailed case investigation in Edo and Ekiti states following recent reports and currently in Rivers State
6.10 NPHCDA, NCDC and partners concluded a micro plan training in Minna, Niger State for the six States (Borno, FCT, Kebbi, Niger, Plateau & Sokoto) implementing Yellow fever Preventive Mass Vaccination Campaign (PMVC) in November/December, 2018.
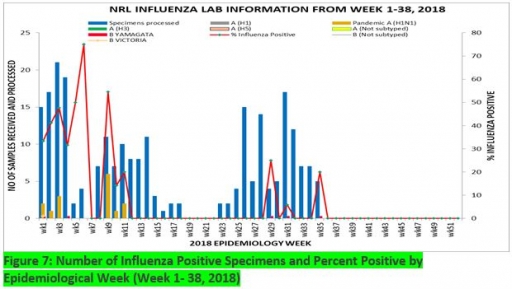
7. Update on national Influenza sentinel surveillance, Nigeria week 1 – 38, 2018
7.1. From week 1- 38, 247-suspected cases were reported, of which 223 were Influenza like-illness (ILI), 24 Severe Acute Respiratory Infection (SARI).
7.2 A total of 247 samples were received and all samples were processed. Of the processed samples, 223(90.3%) were ILI cases, 24 (9.7%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 223 processed ILI samples, 10 (7.0%) was positive for Influenza A; 28(12.6%) positive for Influenza B and 185 (79.4%) were negative.
7.5 For the processed 24 SARI samples, five (20.8%) were positive for Influenza A, 1 (4.2%) was positive for Influenza B, while the remaining 18 (75.0%) were negative.
7.6 44 (17.8%) of the processed 247 samples were positive for Influenza, with 15 (34.1%) of these positive for Influenza A and 29 (65.9%) positive for Influenza B.
7.5. The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for (0.0%), 15 (100.0%) and 0 (0.0%) of the total influenza A positive samples respectively.
7.6 The subtypes B VICTORIA, B Not subtyped and B Yamagata account for 23(79.3%), 5(17.2%) and 1(3.5%) of the total influenza B positive samples respectively
7.7 The percentage influenza positive was highest (75.0%) in week 6, 2018
7.8 In the reporting week 1 -38, all samples were processed in the National Reference Laboratory
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
