The 3rd Annual Disease Surveillance Review Meeting (ADSRM) took place at Bristol Palace Hotel, in Kano state from the 4th - 6th April, 2018. The event brought together all the Surveillance officers in the 36 States and the Federal Capital Territory (FCT) as well as State Laboratory Focal Persons, State Health Educators, Staff of public health laboratories, representatives of programmes & agencies of the Federal Ministries of Health, Agriculture and Rural Development, Environment, development partners in disease control activities and the media. This meeting was organised by the Nigeria Centre for Disease Control (NCDC) in collaboration with her Partners (WHO, US-CDC, University of Maryland Baltimore (UMB), African Field Epidemiology Network (AFENET), Pro Health International, UNICEF and Public Health England(PHE)) with the theme “Transforming Public Health Surveillance and Response: Priorities and innovations’’. Over 200 participants attended.
The opening ceremony was graced by His Excellency the Governor of Kano State represented by the Deputy Governor; Prof Hafiz, Hon. Commissioner for Health Kano State: Dr Kabir Getso, His Eminence the Emir of Kano Sanusi Lamido Sanusi represented by Alhaji Wada Aliyu (Sarkin Yakin Kano) and Director of Public Health Kano State Ministry of Health; Dr Tijjani Husain
Updates were provided by the States as well as partners and NCDC, sharing experiences over the last year, best practice and priorities for the coming year.
1. States to identify priority disease areas and involve partners in utilising parallel program resources for IDSR
2. Advocacy to executives at State and LGA levels should be instituted and maintained for the prompt release of funds
3. States should ensure a budget line and prompt release of funds for surveillance activities, taking full ownership
4. States should identify, designate and equip isolation/treatment centres for infectious diseases
5. Regular after-action review meetings and simulations should be conducted in all states and the FCT
6. States should ensure all health facilities (Public and private) report priority diseases to the LGA DSNOs.
7. States should set up a functional Emergency Operations Centre (EOC) with clear roles and responsibilities
8. NCDC should define the minimum standard requirements for State Epidemiologists, State and LGA DSNOs in Nigeria and also find resources required to achieve this standard
9. Enrollment of Laboratories across states into strengthening Laboratory management accreditation and training on biosecurity/biosafety
10. Training of personnel SLMTA and QMS, ISO 15189 and copies should be distributed to States
11. States to adopt a mechanism ensuring prompt sample transportation from LGAs to State capitals
14. States should identify and empower laboratory focal persons with necessary tools to function with clear roles and responsibilities.
15. NCDC and the State Ministries of Health should urgently identify laboratories at the health facilities that could be utilized in the referral network.
16. Ministry of Agriculture and Rural development should strengthen animal disease surveillance and collaborate with the NCDC
17. Collaborative research between human, animal and environmental health should be strengthened
18. Sustain and scale up the education of communities on preparedness for and prevention of outbreaks
19. Training and retraining of health educators for effective implementation of social and behaviour change communication activities
20. State Teams should integrate communication work plan and scale up campaigns at the grassroots to facilitate early detection and response
These recommendations will be disseminated to all State Commissioners and will form the basis for tracking progress at next year’s annual meeting.
SUMMARY OF REPORTS
In the reporting week ending on March 25, 2018:
o There were 146 new cases of Acute Flaccid Paralysis (AFP) reported. None was confirmed as Polio. The last reported case of Polio in Nigeria was in August 2016. Active case search for AFP is being intensified as Nigeria has reinvigorated its efforts at eradicating Polio.
o 351 suspected cases of Cholera were reported from nine LGAs in seven States (Abia – 13, Bauchi – 289, Borno – 21, Ebonyi – 9, Kaduna – 3, Kano – 15 & Kwara - 1). Of these, six were laboratory confirmed and five deaths were recorded.
o 27 suspected cases of Lassa fever were reported from 12 LGAs in nine States (Bauchi – 3, Edo – 2, Ekiti – 1, FCT – 1, Kogi – 2, Ondo – 13, Osun – 1, Plateau – 2 & Taraba - 2). Six were laboratory confirmed and one death was recorded.
o There were 224 suspected cases of Cerebrospinal Meningitis (CSM) reported from 65 LGAs in 14 States (Adamawa – 4, Bauchi – 1, Benue – 3, Borno – 2, Cross River – 3, Kaduna – 5, Kano – 7, Katsina - 113, Kebbi – 4, Nasarawa – 3, Sokoto – 26, Taraba – 3, Yobe - 3 & Zamfara - 47). Of these, 14 were laboratory confirmed and seven deaths were recorded. Ongoing surveillance for CSM has been intensified in all the 26 States in the Nigeria meningitis belt and case-based surveillance commenced from 4th December 2017
o There were 782 suspected cases of Measles reported from 34 States. Four were laboratory confirmed and 16 deaths were recorded.
In the reporting week, all States sent in their report. Timeliness of reporting remains 86% in both previous & current weeks (week 10 & 11, 2018) while completeness increases from 99% to 100% at the same period. It is very important for all States to ensure timely and complete reporting at all times, especially during an outbreak.
REPORT ANALYSIS AND INTERPRETATION
1. AFP
1.1. As at March 25th, 2018, no new case of WPV was recorded
1.2. In the reporting week, 146 cases of AFP were reported from 121 LGAs in 27 States & FCT
1.2.1. AFP Surveillance has been enhanced and outbreak response is on-going in Borno and other high-risk States
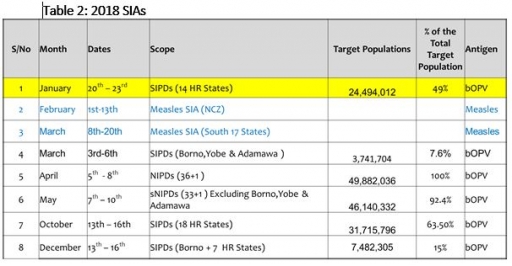
1.2.2. The 1st round of SIPDs in 2018 conducted from 20th – 23rd January 2018 in the 14 high-risk States using bOPV. The schedule for other SIAs is as described in Table 2
1.2.3 The 2nd round of SIPDs conducted from 3rd to 6th of March, 2018 in Borno, Yobe, Adamawa and Zamfara (moved from January round) States using bOPV
1.3. The first round of NIPDs ongoing in the 36 States & FCT from the 7th – 10th April 2018 using bOPV
1.4. Six confirmed WPVs were isolated in 2014.
1.5. The SIAs were strengthened with the following events:
1.5.1. Immunisation for all vaccine-preventable diseases in some selected wards/LGAs.
1.5.2. Use of health camp facilities.
1.5.3. Field supportive supervision and monitoring.
1.5.4. Improved Enhanced Independent Monitoring (EIM) and Lots Quality Assessments (LQAs) in all Polio high-risk States.
1.5.5. High level of an accountability framework
2. CEREBROSPINAL MENINGITIS (CSM)
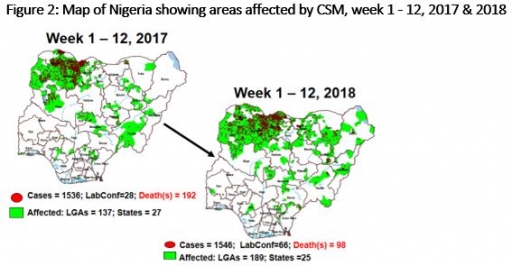
2.1 In the reporting week, 224 suspected Cerebrospinal Meningitis (CSM) cases with 14 Lab. confirmed and seven deaths (CFR, 3.13%) were reported from 65 LGAs (14 States; Adamawa – 4, Bauchi – 1, Benue – 3, Borno – 2, Cross River – 3, Kaduna – 5, Kano – 7, Katsina - 113, Kebbi – 4, Nasarawa – 3, Sokoto – 26, Taraba – 3, Yobe - 3 & Zamfara - 47) compared with 499 suspected cases with three Lab. Confirmed cases and 54 deaths (CFR, 10. 82%) from 58 LGAs (12 States) at the same period in 2017 (Figure 2)
2.2 Between weeks 1 and 12 (2018), 1546 suspected meningitis cases with 66 laboratory confirmed and 98 deaths (CFR, 6.34%) from 189 LGAs (25 States) were reported compared with 1536 suspected cases and 192 deaths (CFR, 12.5%) from 137 LGAs (27 States) during the same period in 2017.
2.3 Timeliness/completeness of CSM case-reporting from States to the National Level (2018 versus 2017): on average, 88.5% of the 26 endemic States sent CSM reports in a timely manner while 95.2% were complete in week 1 - 12, 2018 as against 76.4% timeliness and 92.3% completeness recorded within the same period in 2017
2.4 The National CSM Emergency Operations Centre has been activated and is currently in response mode
2.5 Enhanced surveillance/ case-based surveillance began 1st of December 2017
2.6 Rapid Response Team has been deployed to Niger State
2.7 The National CSM Guidelines have been finalised and available via http://ncdc.gov.ng/themes/common/docs/protocols/51_1510449270.pdf
2.8 State CSM Emergency Operations Centre has been activated in Zamfara, Katsina and Sokoto States respectively
2.9 Preventive vaccination conducted in Yobe State with Men Afrivac in two phases -7th to 11th and 14th to 18th February, 2018
2.10 Reactive vaccination using A, C W135 polysaccharide vaccine carried out in Katsina Central Prison
2.11 A five-day reactive vaccination campaign was concluded in Zamfara State on the 3rd March 2018 in two wards (Birni Magaji & Danfani Sabon Birni) in Birnin Magaji LGA
2.12 NCDC deployed multi-disease response team to Bauchi State on the 11th March 2018 to support the State
2.13 Nigeria procured in-country vaccine to vaccinate Majia ward in Taura LGA, Jigawa State
2.14 NCDC, NPHCDA and partners sent ICG request for 18 wards in six States on the 17th March 2018
2.15 NCDC sent feedback CSM funding need to Nigeria Governors forum
2.16 CSM preventive messages & action were disseminated through a live phone-in discussion programme on a National radio station on the 10th March 2018
2.17 Monitoring of risk communication activities in all States especially high-risk States
2.18 Surveillance Outbreak and Response Management Analysis System (SORMAS) tool deployed in Zamfara, Sokoto and Katsina states
CHOLERA
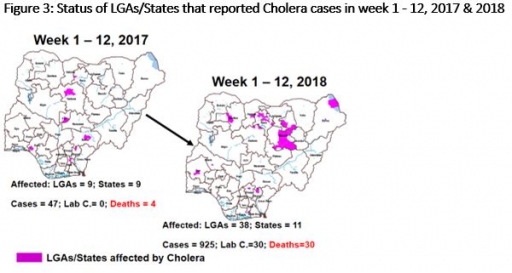
3.1 351 suspected cases of Cholera with six Lab. Confirmed cases and five deaths (CFR, 1.43%) were reported from nine LGAs (seven States; Abia – 13, Bauchi – 289, Borno – 21, Ebonyi – 9, Kaduna – 3, Kano – 15 & Kwara - 1) in week 12, 2018 compared with one case reported from Gombe LGA in Gombe State during the same period in 2017 (Figure 3).
3.2 Between weeks 1 and 12 (2018), 925 suspected Cholera cases with 30 laboratory confirmed and 30 deaths (CFR, 3.24%) from 38 LGAs (11 States) were reported compared with 47 suspected cases and four deaths (CFR, 8.51%) from nine LGAs (nine States) during the same period in 2017.
3.3 National Preparedness and Response to Acute Watery Diarrhoea/ Cholera Guidelines have been finalised: http://ncdc.gov.ng/themes/common/docs/protocols/45_1507196550.pdf
3.4 Ongoing plans for nationwide Cholera campaign with Federal Ministry of Water Resources and partner agencies
3.5 Rapid Response Team deployed to respond to the recent cluster of cases in Bauchi State
LASSA FEVER
Please note that the data reflects the routine reports i.e. all suspected cases including the laboratory positive and negative cases
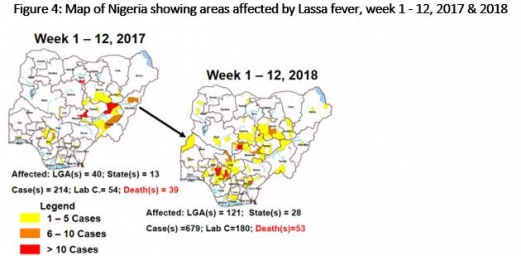
4.1 27 suspected cases of Lassa fever with six Laboratory confirmed and one death (CFR, 3.7%) were reported from 12 LGAs (nine States: Bauchi – 3, Edo – 2, Ekiti – 1, FCT – 1, Kogi – 2, Ondo – 13, Osun – 1, Plateau – 2 & Taraba - 2) in week 12, 2018 compared with 12 suspected cases with four Lab. Confirmed and two death (CFR,16.7%) reported from four LGAs (four States) at the same period in 2017
4.2 Laboratory results of the 27 suspected cases; six positive for Lassa fever (Edo – 2, FCT – 1, Ondo – 2 & Osun - 1), 21 were negative for Lassa fever & other VHFs (Bauchi – 3, Ekiti– 1, Kogi – 2, Ondo – 11, Plateau - 2 & Taraba – 2)
4.3 Between weeks 1 and 12 (2018), 679 suspected Lassa fever cases with 180 laboratory confirmed cases and 53 deaths (CFR, 7.81%) from 121 LGAs (28 States) were reported compared with 214 suspected cases with 54 laboratory confirmed cases and 39 deaths (CFR, 18.22%) from 40 LGAs (13 States) during the same period in 2017 (Figure 4)
4.4 Surveillance Outbreak and Response Management Analysis System (SORMAS) tool deployed in Edo, Ondo and Ebonyi States
4.5 Investigation and active case search ongoing in affected States with coordination of response activities by the NCDC with support from partners
4.6 National Lassa Fever Working Group has been escalated to National Emergency Operations Centre on the 22nd January 2018
4.7 Response materials for VHF provided to support States and health facilities
4.8 National VHF guidelines (National Viral Haemorrhagic Fevers Preparedness guidelines, Infection Prevention and Control of VHF and Standard Operating Procedures for Lassa fever management) are available on the NCDC website- http://ncdc.gov.ng/diseases/guidelines
4.9 NCDC provided Ribavirin and other necessary supportive management to States and their treatment centres
4.10 NCDC Rapid Response Teams currently in Ebonyi, Edo and Ondo States. Risk communications Team deployed to support response
4.11 High-level advocacy and assessment visit by joint NCDC/WHO Team to Edo and Ondo States
4.12 Offsite support provided by NCDC/partners in all affected States
4.13 NCDC in collaboration with ALIMA is providing support to treatment centres in
Ebonyi, Ondo and Edo States where most of the patients are managed
4.13 NCDC deployed data management tools (SORMAS) on the field to encourage real-time reporting and data analysis/interpretation to inform prompt decision making
4.14 NCDC deployed case management teams to Kogi, Bauchi, Taraba and Plateau States
4.15 States are enjoined to intensify surveillance and promote Infection, Prevention and Control (IPC) measures in health facilities
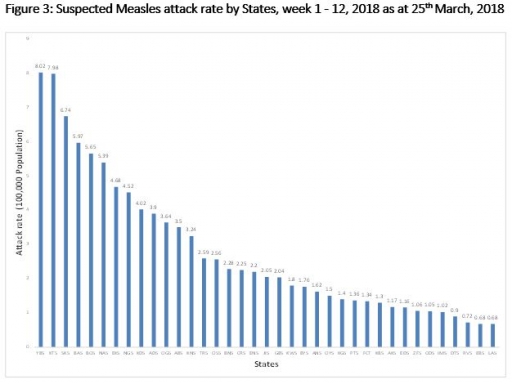
5 MEASLES
5.1 In the reporting week, 782 suspected cases of Measles with four Lab. Confirmed and 16 deaths (CFR, 2.05%) were reported from 34 States compared with 828 suspected cases nine Lab. Confirmed and one death (CFR, 1.21%) reported from 33 States during the same period in 2017
5.2 So far, 5548 suspected Measles cases with six Lab. Confirmed and 50 deaths (CFR, 0.9%) were reported from 36 States and FCT compared with 6631 suspected cases with 51 laboratory confirmed and 39 deaths (CFR, 0.59 %) from 37 States during the same period in 2017
5.3 Response measures include immunization for all vaccine-preventable diseases in some selected/affected wards/LGAs during SIAs, as well as case management
5.4 Measles mass campaign completed in the 17 Southern States from March 8 – 20, 2018
5.5 Measles mass campaign completed in the Northcentral States in February 2018 while North East and the North Western States were conducted in 2017
6 GUINEA WORM DISEASE
6.1 In the reporting week, no rumour report of Guinea Worm disease was received from any State.
6.2 Nigeria has celebrated eight consecutive years of zero reporting of Guinea worm disease in the country. The Country has been officially certified free of Dracunculiasis transmission by the International Commission for the Certification of Dracunculiasis Eradication (ICCDE).
(For further information, contact Nigeria Guinea Worm Eradication Program / Neglected Tropical Diseases Division, Public Health Department/Federal Ministry of Health)
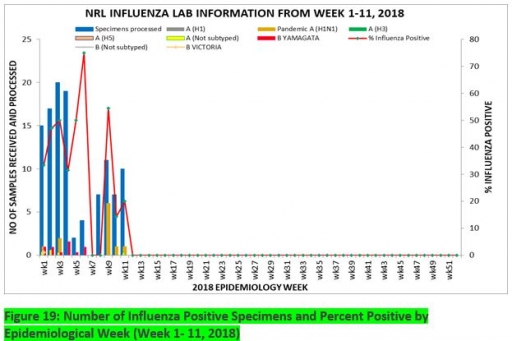
7. Update on national Influenza sentinel surveillance, Nigeria week 1 - 11, 2018
7.1. From week 1- 11, 112-suspected cases were reported, of which 104 were Influenza-like-illness (ILI), eight Severe Acute Respiratory Infection (SARI).
7.2 112 samples were received and all the samples were processed. Of the processed samples, 104(92.9%) were ILI cases, eight (7.1%) were Severe Acute Respiratory Infection (SARI).
7.4. Of the 104 processed ILI samples, 16 (15.4%) was positive for Influenza A; 26(25.0%) positive for Influenza B and 62(59.6%) were negative.
7.5 For the processed eight SARI samples, five (62.5%) were positive for Influenza A while the remaining three (37.5%).were negative.
7.6 42 (37.5%) of the processed 104 samples were positive for Influenza, with 16 (38.1%) of these positive for Influenza A and 26 (62.9%) positive for Influenza B.
7.5. The subtypes A seasonal H3, 2009A/H1N1 and A/not subtyped account for (0.0%), 11 (68.8%) and 5 (31.2%) of total influenza A positive samples respectively.
7.6 The subtypes B VICTORIA, B Not subtyped and B Yamagata account for 10(38.5%), 16(61.5%) and 0(0.0%) of the total influenza B positive samples respectively
7.7 The percentage influenza positive was highest (75.0%) in week 6, 2018
7.8 In the reporting week 1 -11, no samples were left unprocessed
FOR MORE INFORMATION CONTACT
Surveillance Unit:
Nigeria Centre for Disease Control,
801 Ebitu Ukiwe Street, Jabi, Abuja, Nigeria.
[email protected]
www.ncdc.gov.ng/reports
0800-970000-10


 Toll Free Number: 6232
Toll Free Number: 6232 Whatsapp: +234 708 711 0839
Whatsapp: +234 708 711 0839 SMS Number: +234 809 955 5577
SMS Number: +234 809 955 5577 
